ВУЗ: Казахский национальный медицинский университет им. С.Д. Асфендиярова
Категория: Не указан
Дисциплина: Медицина
Добавлен: 05.02.2019
Просмотров: 1337
Скачиваний: 2
Page 6
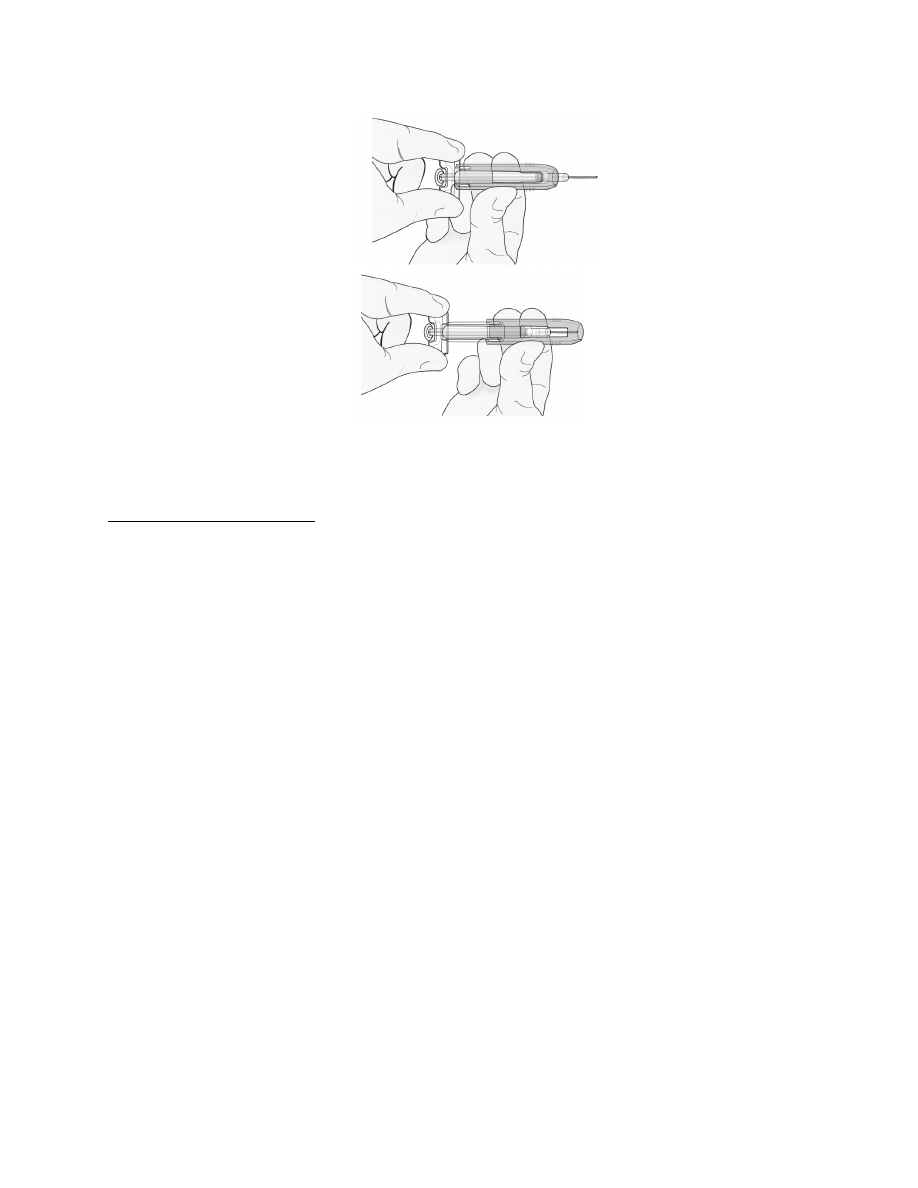
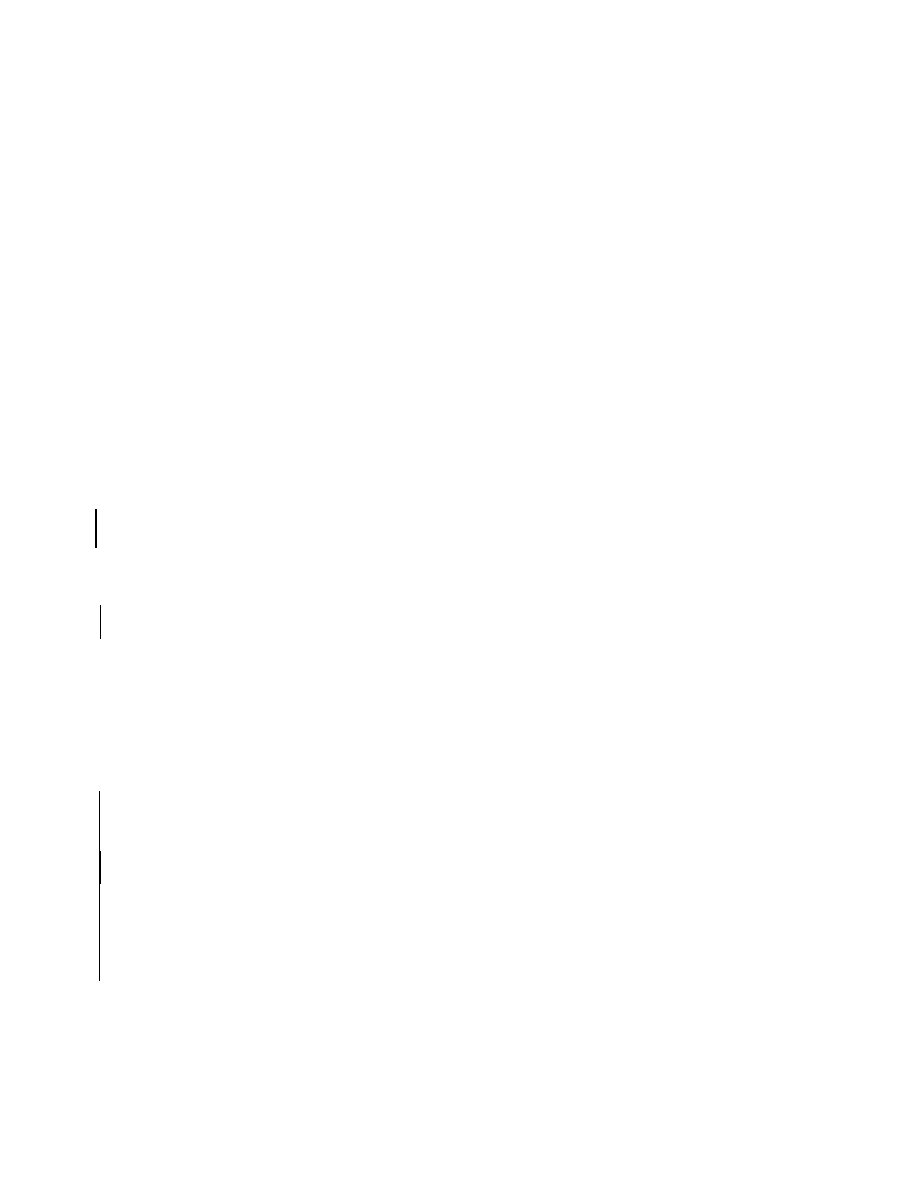
Hold clear finger grip.
Gently slide green safety guard over
needle and lock securely in place. Do
not grip green safety guard too firmly
when sliding over needle.
Immediately dispose of the syringe and needle cap in the nearest sharps container. DO NOT put the
needle cap back on the used syringe.
Instructions for Single-use Vial
For administration of Prolia from the single-use vial, use a 27-gauge needle to withdraw and inject the
1 mL dose. Do not re-enter the vial. Discard vial and any liquid remaining in the vial.
3
DOSAGE FORMS AND STRENGTHS
1 mL of a 60 mg/mL solution in a single-use prefilled syringe
1 mL of a 60 mg/mL solution in a single-use vial
4
CONTRAINDICATIONS
4.1
Hypocalcemia
Pre-existing hypocalcemia must be corrected prior to initiating therapy with Prolia [see Warnings and
Precautions (5.3)].
4.2
Pregnancy
Prolia may cause fetal harm when administered to a pregnant woman. In utero denosumab exposure in
cynomolgus monkeys resulted in increased fetal loss, stillbirths, and postnatal mortality, along with
evidence of absent lymph nodes, abnormal bone growth and decreased neonatal growth. Prolia is
contraindicated in women who are pregnant. If this drug is used during pregnancy, or if the patient
becomes pregnant while taking this drug, the patient should be apprised of the potential hazard to a fetus
[see Use in Specific Populations (8.1)].
4.3
Hypersensitivity
Prolia is contraindicated in patients with a history of systemic hypersensitivity to any component of the
product. Reactions have included anaphylaxis, facial swelling and urticaria [see Warnings and
Precautions (5.2), Adverse Reactions (6.2)].
Page 7
5
WARNINGS AND PRECAUTIONS
5.1
Drug Products with Same Active Ingredient
Prolia contains the same active ingredient (denosumab) found in Xgeva. Patients receiving Prolia should
not receive Xgeva.
5.2
Hypersensitivity
Clinically significant hypersensitivity including anaphylaxis has been reported with Prolia. Symptoms
have included hypotension, dyspnea, throat tightness, facial and upper airway edema, pruritus, and
urticaria. If an anaphylactic or other clinically significant allergic reaction occurs, initiate appropriate
therapy and discontinue further use of Prolia [see Contraindications (4.3), Adverse Reactions (6.2)].
5.3
Hypocalcemia and Mineral Metabolism
Hypocalcemia may be exacerbated by the use of Prolia. Pre-existing hypocalcemia must be corrected
prior to initiating therapy with Prolia. In patients predisposed to hypocalcemia and disturbances of
mineral metabolism (e.g. history of hypoparathyroidism, thyroid surgery, parathyroid surgery,
malabsorption syndromes, excision of small intestine, severe renal impairment [creatinine
clearance < 30 mL/min] or receiving dialysis), clinical monitoring of calcium and mineral levels
(phosphorus and magnesium) is highly recommended within 14 days of Prolia injection. In some
postmarketing cases, hypocalcemia persisted for weeks or months and required frequent monitoring and
intravenous and/or oral calcium replacement, with or without vitamin D.
Hypocalcemia following Prolia administration is a significant risk in patients with severe renal
impairment [creatinine clearance < 30 mL/min] or receiving dialysis. These patients may also develop
marked elevations of serum parathyroid hormone (PTH). Instruct all patients with severe renal
impairment, including those receiving dialysis, about the symptoms of hypocalcemia and the importance
of maintaining calcium levels with adequate calcium and vitamin D supplementation.
Adequately supplement all patients with calcium and vitamin D [see Dosage and Administration (2.1),
Contraindications (4.1), Adverse Reactions (6.1), and Patient Counseling Information (17.3)].
5.4
Osteonecrosis of the Jaw
Osteonecrosis of the jaw (ONJ), which can occur spontaneously, is generally associated with tooth
extraction and/or local infection with delayed healing. ONJ has been reported in patients receiving
denosumab [see Adverse Reactions (6.1)]. A routine oral exam should be performed by the prescriber
prior to initiation of Prolia treatment. A dental examination with appropriate preventive dentistry is
recommended prior to treatment with Prolia in patients with risk factors for ONJ such as invasive dental
procedures (e.g. tooth extraction, dental implants, oral surgery), diagnosis of cancer, concomitant
therapies (e.g. chemotherapy, corticosteroids, angiogenesis inhibitors), poor oral hygiene, and co-morbid
disorders (e.g. periodontal and/or other pre-existing dental disease, anemia, coagulopathy, infection, ill-
fitting dentures). Good oral hygiene practices should be maintained during treatment with Prolia.
Concomitant administration of drugs associated with ONJ may increase the risk of developing ONJ.
For patients requiring invasive dental procedures, clinical judgment of the treating physician and/or oral
surgeon should guide the management plan of each patient based on individual benefit-risk assessment.
Page 8
Patients who are suspected of having or who develop ONJ while on Prolia should receive care by a dentist
or an oral surgeon. In these patients, extensive dental surgery to treat ONJ may exacerbate the condition.
Discontinuation of Prolia therapy should be considered based on individual benefit-risk assessment.
5.5
Atypical Subtrochanteric and Diaphyseal Femoral Fractures
Atypical low-energy or low trauma fractures of the shaft have been reported in patients receiving Prolia
[see Adverse Reactions (6.1)]. These fractures can occur anywhere in the femoral shaft from just below
the lesser trochanter to above the supracondylar flare and are transverse or short oblique in orientation
without evidence of comminution. Causality has not been established as these fractures also occur in
osteoporotic patients who have not been treated with anti-resorptive agents.
Atypical femoral fractures most commonly occur with minimal or no trauma to the affected area. They
may be bilateral and many patients report prodromal pain in the affected area, usually presenting as dull,
aching thigh pain, weeks to months before a complete fracture occurs. A number of reports note that
patients were also receiving treatment with glucocorticoids (e.g. prednisone) at the time of fracture.
During Prolia treatment, patients should be advised to report new or unusual thigh, hip, or groin pain.
Any patient who presents with thigh or groin pain should be suspected of having an atypical fracture and
should be evaluated to rule out an incomplete femur fracture. Patient presenting with an atypical femur
fracture should also be assessed for symptoms and signs of fracture in the contralateral limb. Interruption
of Prolia therapy should be considered, pending a risk/benefit assessment, on an individual basis.
5.6
Serious Infections
In a clinical trial of over 7800 women with postmenopausal osteoporosis, serious infections leading to
hospitalization were reported more frequently in the Prolia group than in the placebo group [see Adverse
Reactions (6.1)]. Serious skin infections, as well as infections of the abdomen, urinary tract, and ear,
were more frequent in patients treated with Prolia. Endocarditis was also reported more frequently in
Prolia-treated patients. The incidence of opportunistic infections was similar between placebo and Prolia
groups, and the overall incidence of infections was similar between the treatment groups. Advise patients
to seek prompt medical attention if they develop signs or symptoms of severe infection, including
cellulitis.
Patients on concomitant immunosuppressant agents or with impaired immune systems may be at
increased risk for serious infections. Consider the benefit-risk profile in such patients before treating with
Prolia. In patients who develop serious infections while on Prolia, prescribers should assess the need for
continued Prolia therapy.
5.7
Dermatologic Adverse Reactions
In a large clinical trial of over 7800 women with postmenopausal osteoporosis, epidermal and dermal
adverse events such as dermatitis, eczema, and rashes occurred at a significantly higher rate in the Prolia
group compared to the placebo group. Most of these events were not specific to the injection site
[see Adverse Reactions (6.1)]. Consider discontinuing Prolia if severe symptoms develop.
5.8
Musculoskeletal Pain
In post-marketing experience, severe and occasionally incapacitating bone, joint, and/or muscle pain has
been reported in patients taking Prolia [see Adverse Reactions (6.2)]. The time to onset of symptoms
Page 9
varied from one day to several months after starting Prolia. Consider discontinuing use if severe
symptoms develop [see Patient Counseling Information (17.8)].
5.9
Suppression of Bone Turnover
In clinical trials in women with postmenopausal osteoporosis, treatment with Prolia resulted in significant
suppression of bone remodeling as evidenced by markers of bone turnover and bone histomorphometry
[see Clinical Pharmacology (12.2) and Clinical Studies (14.1)]. The significance of these findings and
the effect of long-term treatment with Prolia are unknown. The long-term consequences of the degree of
suppression of bone remodeling observed with Prolia may contribute to adverse outcomes such as
osteonecrosis of the jaw, atypical fractures, and delayed fracture healing. Monitor patients for these
consequences.
6
ADVERSE REACTIONS
The following serious adverse reactions are discussed below and also elsewhere in the labeling:
Hypocalcemia [see Warnings and Precautions (5.3)]
Serious Infections [see Warnings and Precautions (5.6)]
Dermatologic Adverse Reactions [see Warnings and Precautions (5.7)]
Osteonecrosis of the Jaw [see Warnings and Precautions (5.4)]
Atypical Subtrochanteric and Diaphyseal Femoral Fractures [see Warnings and Precautions (5.5)]
The most common adverse reactions reported with Prolia in patients with postmenopausal osteoporosis
are back pain, pain in extremity, musculoskeletal pain, hypercholesterolemia, and cystitis.
The most common adverse reactions reported with Prolia in men with osteoporosis are back pain,
arthralgia, and nasopharyngitis.
The most common (per patient incidence ≥ 10%) adverse reactions reported with Prolia in patients with
bone loss receiving androgen deprivation therapy for prostate cancer or adjuvant aromatase inhibitor
therapy for breast cancer are arthralgia and back pain. Pain in extremity and musculoskeletal pain have
also been reported in clinical trials.
The most common adverse reactions leading to discontinuation of Prolia in patients with postmenopausal
osteoporosis are back pain and constipation.
The Prolia Postmarketing Active Safety Surveillance Program is available to collect information from
prescribers on specific adverse events. Please see
r call 1-800-772-6436 for more
information about this program.
6.1
Clinical Trials Experience
Because clinical studies are conducted under widely varying conditions, adverse reaction rates observed
in the clinical studies of a drug cannot be directly compared to rates in the clinical studies of another drug
and may not reflect the rates observed in clinical practice.
Page 10
Treatment of Postmenopausal Women with Osteoporosis
The safety of Prolia in the treatment of postmenopausal osteoporosis was assessed in a 3-year,
randomized, double-blind, placebo-controlled, multinational study of 7808 postmenopausal women aged
60 to 91 years. A total of 3876 women were exposed to placebo and 3886 women were exposed to Prolia
administered subcutaneously once every 6 months as a single 60 mg dose. All women were instructed to
take at least 1000 mg of calcium and 400 IU of vitamin D supplementation per day.
The incidence of all-cause mortality was 2.3% (n = 90) in the placebo group and 1.8% (n = 70) in the
Prolia group. The incidence of nonfatal serious adverse events was 24.2% in the placebo group and
25.0% in the Prolia group. The percentage of patients who withdrew from the study due to adverse events
was 2.1% and 2.4% for the placebo and Prolia groups, respectively.
Adverse reactions reported in ≥ 2% of postmenopausal women with osteoporosis and more frequently in
the Prolia-treated women than in the placebo-treated women are shown in the table below.
Table 1. Adverse Reactions Occurring in ≥ 2% of Patients with Osteoporosis and More Frequently
than in Placebo-treated Patients
SYSTEM ORGAN CLASS
Preferred Term
Prolia
(N = 3886)
n (%)
Placebo
(N = 3876)
n (%)
BLOOD AND LYMPHATIC SYSTEM DISORDERS
Anemia
129 (3.3)
107 (2.8)
CARDIAC DISORDERS
Angina pectoris
101 (2.6)
87 (2.2)
Atrial fibrillation
79 (2.0)
77 (2.0)
EAR AND LABYRINTH DISORDERS
Vertigo
195 (5.0)
187 (4.8)
GASTROINTESTINAL DISORDERS
Abdominal pain upper
129 (3.3)
111 (2.9)
Flatulence
84 (2.2)
53 (1.4)
Gastroesophageal reflux disease
80 (2.1)
66 (1.7)
GENERAL DISORDERS AND ADMINISTRATION
SITE CONDITIONS
Edema peripheral
189 (4.9)
155 (4.0)
Asthenia
90 (2.3)
73 (1.9)
INFECTIONS AND INFESTATIONS
Cystitis
228 (5.9)
225 (5.8)
Upper respiratory tract infection
190 (4.9)
167 (4.3)
Pneumonia
152 (3.9)
150 (3.9)