ВУЗ: Казахский национальный медицинский университет им. С.Д. Асфендиярова
Категория: Не указан
Дисциплина: Медицина
Добавлен: 05.02.2019
Просмотров: 1555
Скачиваний: 2
Page 21
Table 2. The Effect of Prolia on the Incidence of
New Vertebral Fractures in Postmenopausal Women
Proportion of Women
With Fracture (%)
+
Absolute Risk
Reduction
(%)
*
(95% CI)
Relative Risk
Reduction
(%)
*
(95% CI)
Placebo
N = 3691
(%)
Prolia
N = 3702
(%)
0-1 Year
2.2
0.9
1.4 (0.8, 1.9)
61 (42, 74)
0-2 Years
5.0
1.4
3.5 (2.7, 4.3)
71 (61, 79)
0-3 Years
7.2
2.3
4.8 (3.9, 5.8)
68 (59, 74)
+
Event rates based on crude rates in each interval.
*
Absolute risk reduction and relative risk reduction based on Mantel-Haenszel method adjusting for age
group variable.
Prolia was effective in reducing the risk for new morphometric vertebral fractures regardless of age,
baseline rate of bone turnover, baseline BMD, baseline history of fracture, or prior use of a drug for
osteoporosis.
Effect on Hip Fractures
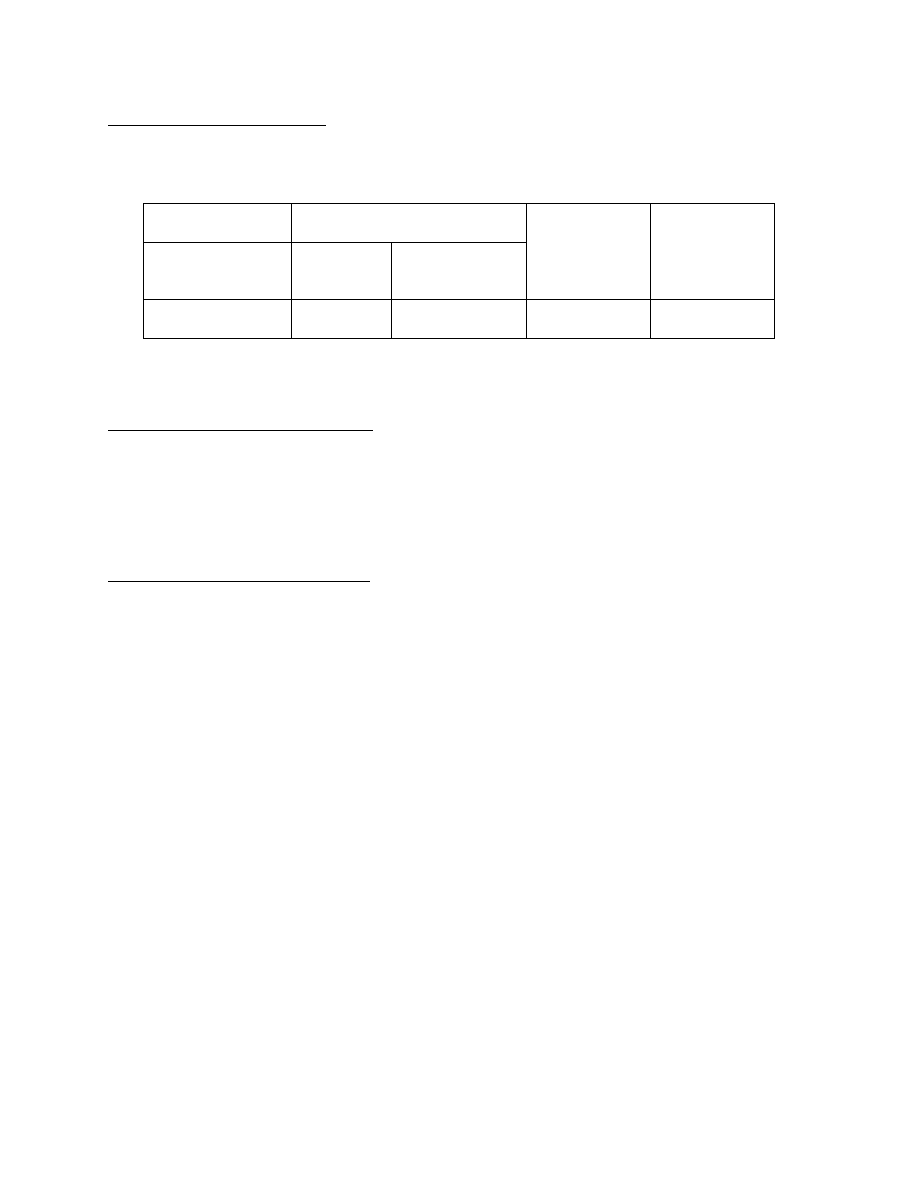
The incidence of hip fracture was 1.2% for placebo-treated women compared to 0.7% for Prolia-treated
women at year 3. The age-adjusted absolute risk reduction of hip fractures was 0.3% with a relative risk
reduction of 40% at 3 years (p = 0.04) (Figure 1).
Figure 1. Cumulative Incidence of Hip Fractures Over 3 Years
N = number of subjects randomized
0
2
4
6
8
10
Figure 1-1. Cumulative Incidence of Hip Fractures Over 3 Years
Source Data: a030216.asleff
Output: f1-01-2011mop-uspi-km-ahpfx-216-l.cgm (Date Generated: 10OCT2011:12:38:57)
Program: /stat/amg162/meta/bla_2011maleosteo/analysis/uspi/figures/program/f-km-ahpfx-216.sas
P
a
ti
en
t
H
ip
F
rac
tu
re
I
n
ci
d
en
ce
(
%
)
Study Month
Placebo (N = 3906)
Prolia (N = 3902)
0
6
12
18
24
30
36
0
6
12
18
24
30
36
Page 22
Effect on Nonvertebral Fractures
Treatment with Prolia resulted in a significant reduction in the incidence of nonvertebral fractures
(Table 3).
Table 3. The Effect of Prolia on the Incidence of Nonvertebral Fractures at Year 3
Proportion of Women With
Fracture (%)
+
Absolute Risk
Reduction (%)
(95% CI)
Relative Risk
Reduction (%)
(95% CI)
Placebo
N = 3906
(%)
Prolia
N = 3902
(%)
Nonvertebral
fracture
1
8.0
6.5
1.5 (0.3, 2.7)
20 (5, 33)
*
+
Event rates based on Kaplan-Meier estimates at 3 years.
1
Excluding those of the vertebrae (cervical, thoracic, and lumbar), skull, facial, mandible, metacarpus, and finger and toe
phalanges.
*
p-value = 0.01.
Effect on Bone Mineral Density (BMD)
Treatment with Prolia significantly increased BMD at all anatomic sites measured at 3 years. The
treatment differences in BMD at 3 years were 8.8% at the lumbar spine, 6.4% at the total hip, and 5.2% at
the femoral neck. Consistent effects on BMD were observed at the lumbar spine, regardless of baseline
age, race, weight/body mass index (BMI), baseline BMD, and level of bone turnover.
After Prolia discontinuation, BMD returned to approximately baseline levels within 12 months.
Bone Histology and Histomorphometry
A total of 115 transiliac crest bone biopsy specimens were obtained from 92 postmenopausal women with
osteoporosis at either
month 24 and/or month 36 (53 specimens in Prolia group, 62 specimens in placebo
group). Of the biopsies obtained, 115 (100%) were adequate for qualitative histology and 7 (6%) were
adequate for full quantitative histomorphometry assessment.
Qualitative histology assessments showed normal architecture and quality with no evidence of
mineralization defects, woven bone, or marrow fibrosis in patients treated with Prolia.
The presence of double tetracycline labeling in a biopsy specimen provides an indication of active bone
remodeling, while the absence of tetracycline label suggests suppressed bone formation. In patients
treated with Prolia, 35% had no tetracycline label present at the month 24 biopsy and 38% had no
tetracycline label present at the month 36 biopsy, while 100% of placebo-treated patients had double label
present at both time points. When compared to placebo, treatment with Prolia resulted in virtually absent
activation frequency and markedly reduced bone formation rates. However, the long-term consequences
of this degree of suppression of bone remodeling are unknown.
14.2
Treatment to Increase Bone Mass in Men with Osteoporosis
The efficacy and safety of Prolia in the treatment to increase bone mass in men with osteoporosis was
demonstrated in a 1-year, randomized, double-blind, placebo-controlled trial. Enrolled men had a baseline
BMD T-score between -2.0 and -3.5 at the lumbar spine or femoral neck. Men with a BMD T-score
between -1.0 and -3.5 at the lumbar spine or femoral neck were also enrolled if there was a history of
prior fragility fracture. Men with other diseases (such as rheumatoid arthritis, osteogenesis imperfecta,
and Paget’s disease) or on therapies that may affect bone were excluded from this study. The 242 men
enrolled in the study ranged in age from 31 to 84 years with a mean age of 65 years. Men were
randomized to receive SC injections of either placebo (n = 121) or Prolia 60 mg (n = 121) once every
Page 23
6 months. All men received at least 1000 mg calcium and at least 800 IU vitamin D supplementation
daily.
Effect on Bone Mineral Density (BMD)
The primary efficacy variable was percent change in lumbar spine BMD from baseline to 1 year.
Secondary efficacy variables included percent change in total hip, and femoral neck BMD from baseline
to 1 year.
Treatment with Prolia significantly increased BMD at 1 year. The treatment differences in BMD at 1 year
were 4.8% (+0.9% placebo, +5.7% Prolia; (95% CI: 4.0, 5.6); p < 0.0001) at the lumbar spine, 2.0%
(+0.3% placebo, +2.4% Prolia) at the total hip, and 2.2% (0.0% placebo, +2.1% Prolia) at femoral neck.
Consistent effects on BMD were observed at the lumbar spine regardless of baseline age, race, BMD,
testosterone concentrations and level of bone turnover
.
Bone Histology and Histomorphometry
A total of 29 transiliac crest bone biopsy specimens were obtained from men with osteoporosis at
12 months (17 specimens in Prolia group, 12 specimens in placebo group). Of the biopsies obtained,
29 (100%) were adequate for qualitative histology and, in Prolia patients, 6 (35%) were adequate for full
quantitative histomorphometry assessment. Qualitative histology assessments showed normal
architecture and quality with no evidence of mineralization defects, woven bone, or marrow fibrosis in
patients treated with Prolia. The presence of double tetracycline labeling in a biopsy specimen provides
an indication of active bone remodeling, while the absence of tetracycline label suggests suppressed bone
formation. In patients treated with Prolia, 6% had no tetracycline label present at the month 12 biopsy,
while 100% of placebo-treated patients had double label present. When compared to placebo, treatment
with Prolia resulted in markedly reduced bone formation rates. However, the long-term consequences of
this degree of suppression of bone remodeling are unknown.
14.3
Treatment of Bone Loss in Men with Prostate Cancer
The efficacy and safety of Prolia in the treatment of bone loss in men with nonmetastatic prostate cancer
receiving androgen deprivation therapy (ADT) were demonstrated in a 3-year, randomized (1:1), double-
blind, placebo-controlled, multinational study. Men less than 70 years of age had either a BMD T-score
at the lumbar spine, total hip, or femoral neck between -1.0 and -4.0, or a history of an osteoporotic
fracture. The mean baseline lumbar spine BMD T-score was -0.4, and 22% of men had a vertebral
fracture at baseline. The 1468 men enrolled ranged in age from 48 to 97 years (median 76 years). Men
were randomized to receive subcutaneous injections of either placebo (n = 734) or Prolia 60 mg (n = 734)
once every 6 months for a total of 6 doses. Randomization was stratified by age (< 70 years vs. ≥ 70
years) and duration of ADT at trial entry (≤ 6 months vs. > 6 months). Seventy-nine percent of patients
received ADT for more than 6 months at study entry. All men received at least 1000 mg calcium and
400 IU vitamin D supplementation daily.
Effect on Bone Mineral Density (BMD)
The primary efficacy variable was percent change in lumbar spine BMD from baseline to month 24. An
additional key secondary efficacy variable was the incidence of new vertebral fracture through month 36
diagnosed based on x-ray evaluation by two independent radiologists. Lumbar spine BMD was higher at
2 years in Prolia-treated patients as compared to placebo-treated patients [-1.0% placebo, +5.6% Prolia;
treatment difference 6.7% (95% CI: 6.2, 7.1); p < 0.0001].
With approximately 62% of patients followed for 3 years, treatment differences in BMD at 3 years were
7.9% (-1.2% placebo, +6.8% Prolia) at the lumbar spine, 5.7% (-2.6% placebo, +3.2% Prolia) at the total
hip, and 4.9% (-1.8% placebo, +3.0% Prolia) at the femoral neck. Consistent effects on BMD were
Page 24
observed at the lumbar spine in relevant subgroups defined by baseline age, BMD, and baseline history of
vertebral fracture.
Effect on Vertebral Fractures
Prolia significantly reduced the incidence of new vertebral fractures at 3 years (p = 0.0125), as shown in
Table 4.
Table 4. The Effect of Prolia on the Incidence of
New Vertebral Fractures in Men with Nonmetastatic Prostate Cancer
Proportion of Men With
Fracture (%)
+
Absolute Risk
Reduction
(%)
*
(95% CI)
Relative Risk
Reduction
(%)
*
(95% CI)
Placebo
N = 673
(%)
Prolia
N = 679
(%)
0-1 Year
1.9
0.3
1.6 (0.5, 2.8)
85 (33, 97)
0-2 Years
3.3
1.0
2.2 (0.7, 3.8)
69 (27, 86)
0-3 Years
3.9
1.5
2.4 (0.7, 4.1)
62 (22, 81)
+
Event rates based on crude rates in each interval.
*
Absolute risk reduction and relative risk reduction based on Mantel-Haenszel method adjusting for age
group and ADT duration variables.
14.4
Treatment of Bone Loss in Women with Breast Cancer
The efficacy and safety of Prolia in the treatment of bone loss in women receiving adjuvant aromatase
inhibitor (AI) therapy for breast cancer was assessed in a 2-year, randomized (1:1), double-blind, placebo-
controlled, multinational study. Women had baseline BMD T-scores between -1.0 to -2.5 at the lumbar
spine, total hip, or femoral neck, and had not experienced fracture after age 25. The mean baseline
lumbar spine BMD T-score was -1.1, and 2.0% of women had a vertebral fracture at baseline. The
252 women enrolled ranged in age from 35 to 84 years (median 59 years). Women were randomized to
receive subcutaneous injections of either placebo (n = 125) or Prolia 60 mg (n = 127) once every
6 months for a total of 4 doses. Randomization was stratified by duration of adjuvant AI therapy at trial
entry (≤ 6 months vs. > 6 months). Sixty-two percent of patients received adjuvant AI therapy for more
than 6 months at study entry. All women received at least 1000 mg calcium and 400 IU vitamin D
supplementation daily.
Effect on Bone Mineral Density (BMD)
The primary efficacy variable was percent change in lumbar spine BMD from baseline to month 12.
Lumbar spine BMD was higher at 12 months in Prolia-treated patients as compared to placebo-treated
patients [-0.7% placebo, +4.8% Prolia; treatment difference 5.5% (95% CI: 4.8, 6.3); p < 0.0001].
With approximately 81% of patients followed for 2 years, treatment differences in BMD at 2 years were
7.6% (-1.4% placebo, +6.2% Prolia) at the lumbar spine, 4.7 % (-1.0% placebo, +3.8% Prolia) at the total
hip, and 3.6% (-0.8% placebo, +2.8% Prolia) at the femoral neck.
16
HOW SUPPLIED/STORAGE AND HANDLING
Prolia is supplied in a single-use prefilled syringe with a safety guard or in a single-use vial. The grey
needle cap on the single-use prefilled syringe contains dry natural rubber (a derivative of latex).
60 mg/1 mL in a single-use prefilled syringe
1 per carton
NDC 55513-710-01
60 mg/1 mL in a single-use vial
1 per carton
NDC 55513-720-01

Page 25
Store Prolia in a refrigerator at 2°C to 8°C (36°F to 46°F) in the original carton.
Do not freeze. Prior to
administration, Prolia may be allowed to reach room temperature (up to 25°C/77°F) in the original
container. Once removed from the refrigerator, Prolia must not be exposed to temperatures above
25°C/77°F and must be used within 14 days. If not used within the 14 days, Prolia should be discarded.
Do not use Prolia after the expiry date printed on the label.
Protect Prolia from direct light and heat.
Avoid vigorous shaking of Prolia.
17
PATIENT COUNSELING INFORMATION
See FDA-approved patient labeling (Medication Guide).
17.1
Drug Products with Same Active Ingredient
Advise patients that denosumab is also marketed as Xgeva, and if taking Prolia, they should not receive
Xgeva [see Warnings and Precautions (5.1)].
17.2
Hypersensitivity
Advise patients to seek prompt medical attention if signs or symptoms of hypersensitivity reactions occur.
Advise patients who have had signs or symptoms of systemic hypersensitivity reactions that they should
not receive denosumab (Prolia or Xgeva) [see Warnings & Precautions (5.2), Contraindications (4.3)].
17.3
Hypocalcemia
Adequately supplement patients with calcium and vitamin D and instruct them on the importance of
maintaining serum calcium levels while receiving Prolia [see Warnings and Precautions (5.3) and Use in
Specific Populations (8.6)]. Advise patients to seek prompt medical attention if they develop signs or
symptoms of hypocalcemia.
17.4
Osteonecrosis of the Jaw
Advise patients to maintain good oral hygiene during treatment with Prolia and to inform their dentist
prior to dental procedures that they are receiving Prolia. Patients should inform their physician or dentist
if they experience persistent pain and/or slow healing of the mouth or jaw after dental surgery
[see Warnings and Precautions (5.4)].
17.5
Atypical Subtrochanteric and Diaphyseal Femoral Fractures
Advise patients to report new or unusual thigh, hip, or groin pain [see Warnings and Precautions (5.5)].
17.6
Serious Infections
Advise patients to seek prompt medical attention if they develop signs or symptoms of infections,
including cellulitis [see Warnings and Precautions (5.6)].
17.7
Dermatologic Reactions
Advise patients to seek prompt medical attention if they develop signs or symptoms of dermatological
reactions (dermatitis, rashes, and eczema) [see Warnings and Precautions (5.7)].