Файл: Соколова 2018 скабиозная эритродермия .Scabious-SokolovaTV.pdf
ВУЗ: Московский государственный университет пищевых производств
Категория: Не указан
Дисциплина: Не указана
Добавлен: 07.02.2019
Просмотров: 686
Скачиваний: 2
Our Dermatology Online
© Our Dermatol Online 4.2018
355
How to cite this article:
Sokolova TV, Adaskevich UP, Malyarchuk AP, Lopatina YV. Scabious erythroderma - a rare clinical variant of scabies. Our Dermatol
Online. 2018;9(4):355-362.
Submission:
16.01.2018;
Acceptance:
10.05.2018
DOI:
10.7241/ourd.20184.1
Scabious erythroderma - a rare clinical variant of
Scabious erythroderma - a rare clinical variant of
scabies
scabies
Tatyana V. Sokolova
1
, Uladzimir P. Adaskevich
2
, Alexander P. Malyarchuk
1
,
Yulia V. Lopatina
3
1
Department of Skin and Venerial Diseases and Cosmetology, Medical Institute of Post-Graduate Education, Federal State
Educational Institution of Higher Professional Education "Moscow State University of Food Production", Moscow, Russian
Federation,
2
Department of Dermatovenereology, Vitebsk State Medical University, Vitebsk, Belarus,
3
Department of
Entomology, Biological Faculty, M.V. Lomonosov Moscow State University, Moscow, Russian Federation
Corresponding author:
Prof. Uladzimir P. Adaskevich, E-mail: vitebsk.derma@mail.ru
INTRODUCTION
Erythroderma is an inflammatory skin condition
characterized by erythema and exfoliative dermatitis
involving 90% and more of the entire skin surface.
The initial lesions which are important keys for
understanding the disease evolution are often
occult [1]. The most common causes of erythroderma
can include pre-existing dermatoses (psoriasis,
atopic dermatitis, eczema, seborrhoeic dermatitis,
lichen ruber pilaris, lichen ruber planus, pemphigus
foliaceus, bullous pemphigoid), drug-induced eruption,
lymphoma and leukemia, visceral neoplasias and other
conditions [1-4].
Erythroderma is also a diagnostically relevant clinical
manifestation of Norwegian scabies [1,5,6]. The latter
was first described by Danielson and Boeck in Norway
in 1848. Crusted scabies is another term used to name
this condition. This name reflects the main clinical
symptom of the disease – massive crusts which are
formed in various areas of the skin surface. In addition
to crusts and erythroderma, Norwegian scabiesis
characterized by multiple burrow tracks, polymorphous
eruption (papules, vesicles, pustules) and scales.
The etiology and peculiarities of the disease evolution
have been quite competently systemized [5,7]. For the
last two decades the cases of Norwegian scabies have
ABSTRACT
Background: Erythroderma (exfoliative dermatitis) is an emergency condition in dermatology in which not less than 90%
of skin surface is affected. The presenting features are erythema, skin scaling and itching, fever and lymphadenopathy.
The most common cause of erythroderma is a preexisting dermatosis (psoriasis, atopic dermatitis, eczema, seborheic
dermatitis, lichen rubra pilaris, lichen planus, pemphigus foliaceous), drug reactions, lymphoma, leukemia and visceral
neoplasias. Erythroderma is a diagnostically relevant presenting feature of Norwegian scabies. The aim of investigation: Is
to describe clinical peculiarities of scabious erythroderma as a special rare form of scabies, to assess the number of scabies
mites on the patient and in his/her environment and to work out the criteria of differential diagnosis with Norwegian
scabies. Material and methods: We examined 5 patients with scabies and erythroderma as the main presenting
feature. All patients were women aged from 42 to 89 years. The disease duration was from 8 months to 1 year. The
causes of erythroderma were variable. Clinical and paraclinical methods of investigation alongside with dermatoscopy
and microscopy were used. Results This is the description of a rare clinical form of scabies, scabious erythroderma.
It is based on the analysis of the 5 cases of scabies, whose main clinical manifestation is diffuse erythroderma. The
diagnostic criterias of scabious erythroderma and differential diagnosis of Norwegian scabies are given. The invasive
potential of this form of the disease on the patient and beyond is evaluated for the first time.
Key words:
Scabious erythroderma; Norwegian scabies; Dermatoscopy; The differential diagnosis
Original
Article

www.odermatol.com
© Our Dermatol Online 4.2018
356
been described in HIV-infected patients [8-11], in
elderly and disabled people [12,13] and rarely observed
in cases of brain astrozytoma [14], drug addiction [15],
Down syndrome, diffuse fatty liver disease, anemia,
parenchymatous dystrophy of visceral organs,
cachexia [16], bullous pemphigoid treated with systemic
c orticosteroids [17], congenital erythroderma [18],
in patients taking novel immunosuppressive agents
tozilisumab [19] and cyclosporine [20], in case of skin
exposure to pesticides [21]. Rare cases of Norwegian
scabies are also described without associated pathology:
in a 24-year-old man [22], in a pregnant woman [23],
in children [24,25].
Massive crusts are the main symptom of Norwegian
scabies. Their thickness varies from several millimeters
to 2-3 cm. In some cases crust layers may cover
considerable areas of the skin surface forming a solid
horny shield which limits body movements and makes
thempainful. The crust colour varies greatly from
dirty gray with a mixture of blood to yellowish-green,
grayish-brown or alabaster-white. The crust surface is
rough, fissured and covered with verrucous rupia-like
proliferations. Crusts usually appear at the preferable
sites of burrows (hands, feet, elbows, buttocks and
other localizations). The upper crust layer is firm,
the lower one is friable. Between these two layers a
great amount of adult and immature mites can be
found. On the inner crust surface one can see tortuous
depressions which correspond to scabies mite burrows.
The crusts firmly adhere to the skin surface and, if
forcibly removed, leave large weeping erosions. The
burrows with in the crusts are “many-storied”. In the
lower crustose layers, male and female mites, nymphs,
larvae and eggs can be detected, and in the deep inner
layers, dead mites and eggs, as well as empty egg shells
are found. The number of mites on a sick patient is
immense, so the Norwegian scabies is highly contagious
with local epidemics breaking out around the patient.
Erythroderma is the second diagnostically relevant
symptom of Norwegian scabies [6,13,16,26-31]. The
cause of erythroderma in this case is considered to be
Staphylococcus aureus colonizing mite burrows [32,33].
Staphylococcus aureus was found in mite burrows
of an elderly patient with Norwegien scabies by
scanning electron microscopy, bacterial analysis of
burrow contents revealed Staphylococcus aureus and
Staphylococcus haemolyticus. [34]. It is important to
note the observation suggesting that erythroderma in
Norwegian scabies arising on the background of both
systemic and topical corticosteroid therapies appears
earlier than in case when corticosteroid therapy is not
administered [35,36].
Other diagnostically relevant criteria of Norwegian
scabies are affected nails (nailplates easily crumble,
they are grey with abumpy surface and not chededges,
sometimes nail plates are completely lost and replaced
by massive epidermal crustlike layers); enlargement
of multiple lymph nodes (polyadenopathy); fever
during the entire course of the disease; palmar-plantar
hyperkeratosis; hair changes (dry, dull, ash-gray) up
to alopecia; body malodour (reminiscent of sour
dough) [6,26-31,37].
There are some case reports in medical literature
describing highly contagious scabies with extensive
erythroderma as the main clinical symptom [38,39].
This rare erythrodermic form of scabies is still
insufficiently described in medical literature. That is
why some authors, having found areas of hyperkeratosis
(which are no crusts actually), diagnose such cases as
Norwegian scabies [38-42]. In fact, the given form of the
disease should be designated as scabious erythroderma.
One can assume that there must be far more similar
cases. Besides, it is recognized that Norwegian scabies
may have a localized form with crusts developing only
in certain areas of the skin surface [7,41,42].
The aim of our study was to describe peculiarities
of the clinical course of scabious erythroderma as an
independent rare variant of scabies, to estimate the
number of mites on patients and in their surroundings
and to work out criteria of differential diagnostics with
Norwegian scabies.
MATERIALS AND METHODS
We observed 5 patients with scabies in whom
erythroderma was the main clinical manifestation
of the disease. All patients were women aged 42, 72,
76, 84 and 89. The duration of the disease was from
8 months to 1 year. The causes of the disorder were
different in all the patients. The condition in the first
patient (aged 42) developed on the background of
systemic lupus erythematous. The complex therapy of
this disease included prednisolone 60 mg/day during
3 months. In two patients (aged 72 and 76) allergic
contact dermatitis and then drug-induced reaction
were erroneously diagnosed. During 8-9 months the
patients received systemic antihistamine, desensitizing
drugs and topical glucocorticosteroids. Erythroderma
www.odermatol.com
© Our Dermatol Online 4.2018
357
appeared two months after topical application of
corticosteroids. The forth case was a 84-year-old
patient of psychoneurologic department. Many years
the patient took systemic psychotropic drugs for
schizophrenia, fluocinolon acetonide was applied
topically. The fifth patient (aged 89), in whom allergic
dermatitis and then drug-induced reaction were
diagnosed, received systemic antihistamine drugs,
topical corticosteroids during one year and then
three-month course of betamethasone. Erythroderma
appeared after 2 months of betamethasone injections.
In all cases the diagnosis of scabies was confirmed
by laboratory investigations. The laboratory methods
included mite removal with the help of a needle,
burrow and lesional skin scrapings with lactic acid
application, dermatoscopy performed with the help
of the dermatoscope DELTA 20 and microscopy
with USB-microscopes of various modifications. The
number of burrows was counted visually and by means
of dermatoscopy and then the parasitary index was
determined. In the fifth patient the number of mites on
the apparently normal skin and in erythrodermic lesions
was counted in the field of a standard dermatoscope
with the area of 1 cm
2
. The efficacy of scabies
diagnostics by means of dermatoscopy and tape-test
methods [43,44] was compared. In case of a tape test,
a piece of transparent adhesive Scotch tape (2x5 cm)
was applied on an affected site of the skin for several
seconds and then quickly removed. The removed
piece of tape was paced on the slide and viewed with
the microscope. The quantities of mites in different
stages of development were compared in two epidermal
scrapings (from the abdomen and thigh) and in 4
Scotch-tests (from the foot, chest, back, thigh). The
number of mites around the patient was determined on
the sheet where the patient was lying. For this purpose
the adhesive tape (2x5 cm) was applied to ten different
sites on the sheet.
As an example we describe a case of a patient with
scabious erythroderma diagnosed in June 2013
(Figs. 1-6). A 89-year-old patient admitted to hospital
complained of the affection of the whole skin,
moderate itch increasing in the evening and chills
(in spite of high environmental temperature). The
disease had lasted for one year. The patient did not
connect any events with the onset of the disease and
considered the skin changes to be a result of “allergy”
(she had previously worked as a nurse). The first
symptom of the disease was itch in the interscapular
region. The itching sensation then gradually spread to
other skin regions. The patient’s daughter who cared
for her mother also complained of slight itch. Both
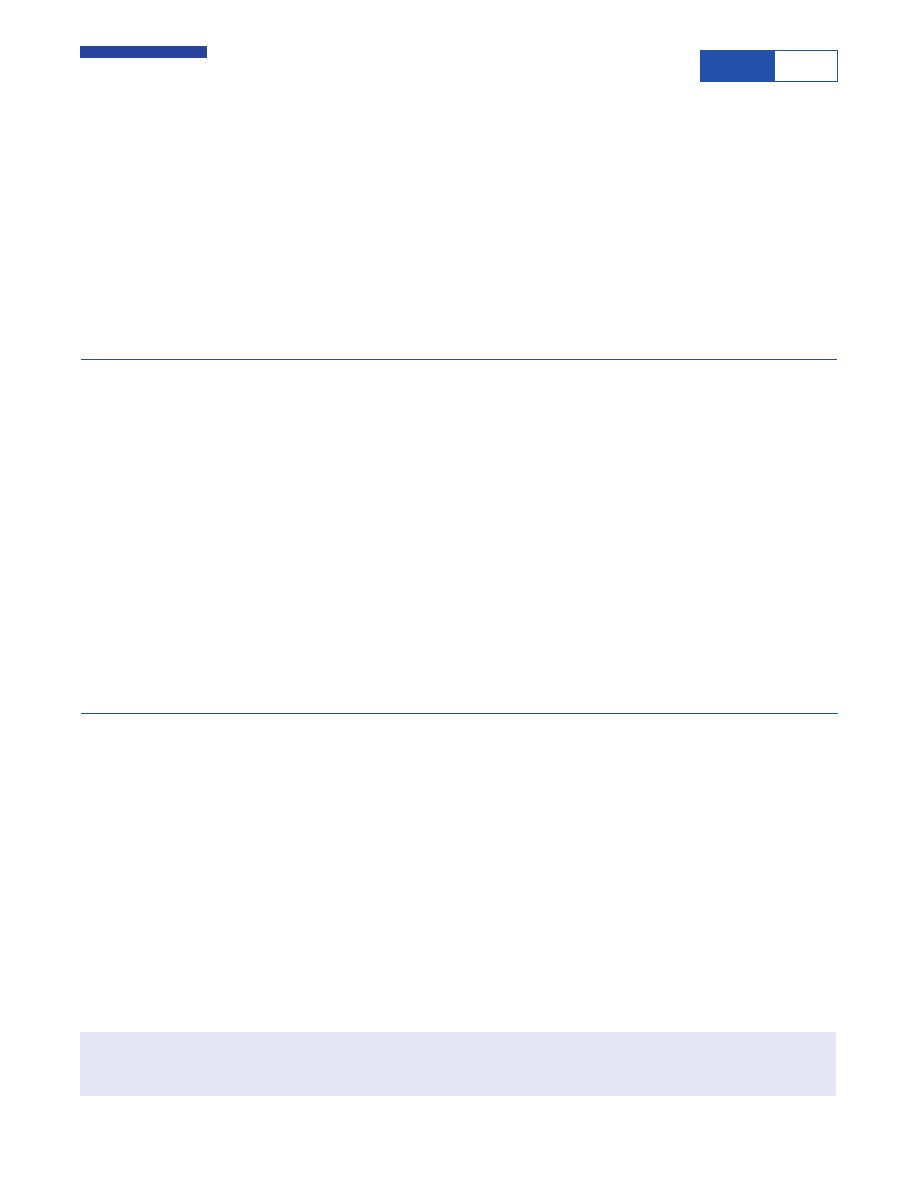
Figure 1:
Focal hyperkeratosis on the buttocks in scabious
erythroderma.
Figure 2:
Mite burrows on the scalp at the frontal hair line in scabious
erythroderma.
Figure 3:
Mite burrows in the interscapular region in scabious
erythroderma.
www.odermatol.com
© Our Dermatol Online 4.2018
358
women took antihistamine drugs and applied topical
medicines against pruritus with no effects after this
self-treatment. On admission to hospital the condition
of the old patient was diagnosed as wide-spread allergic
dermatitis. The patient was treated with antihistamine
and desensitizing drugs and topical corticosteroid
creams. Short-termin significant improvement
was observed. The patient applied to 4 different
doctors but the diagnosis remained the same and the
treatment did not significantly differ from the previous
one. The therapeutic measures brought no effect.
Three months before admission to hospital the patient
was administered 2 injections of betamethasone per
month and topical corticosteroid creams (clobetasol,
fluticasone). While the subjective perception of itch
reduced, there appeared lesions of erythema which
quickly spread and covered the whole skin surface
creating the clinical picture of erythroderma. With
the diagnosis “drug-induced eruption” the patient
was admitted to hospital. The patient’s condition on
admission was satisfactory, the body temperature was
normal. The state of the inner organs and the revealed
pathology in general corresponded to the advanced age
of the patient. The regional lymphnodes were painless
and not enlarged.
Local status. The process was of a universal character
with erythroderma covering the whole skin surface
of the body. The skin was dusky red, dry and in some
areas scaling with signs of infiltration, pigmentation
and lichenification. The skin felt warm, firm and
rough. White dermographism was observed, but
crusts were absent. In the areas of the intergluteal
cleft (Fig. 1) and elbows there were foci of grey
hyperkeratosis with firmly adherent scales. Scratch
marks were hardly present. On the background of
moderate facial hyperemia there were red infiltrated
lesions on the forehead, chin, eyelids, ears, cheeks, and
the vermillion border of the lips. The skin of the scalp
was pale without any signs of inflammation. On the
skin of the shoulders and lower legs there were small
isles of normal skin. The inflammatory changes of the
palmar and plantar surfaces were insignificant. Multiple
fresh and destroyed burrows of various lengths were
observed predominantly in the skin folds. The number
of burrows detected without using a dermatoscope
made up 186 on the palms, 81 on the soles and 34 on
the areolas. Burrows in other skin regions were poorly
visualized without a dermatoscope.
Laboratory data. Moderately elevated WBC count
(13,6×10
9
/L), ESR 3 mm/h, hypoproteinemia 52 g/L.
Other blood biochemistry values and urine analysis
were within the normal range.
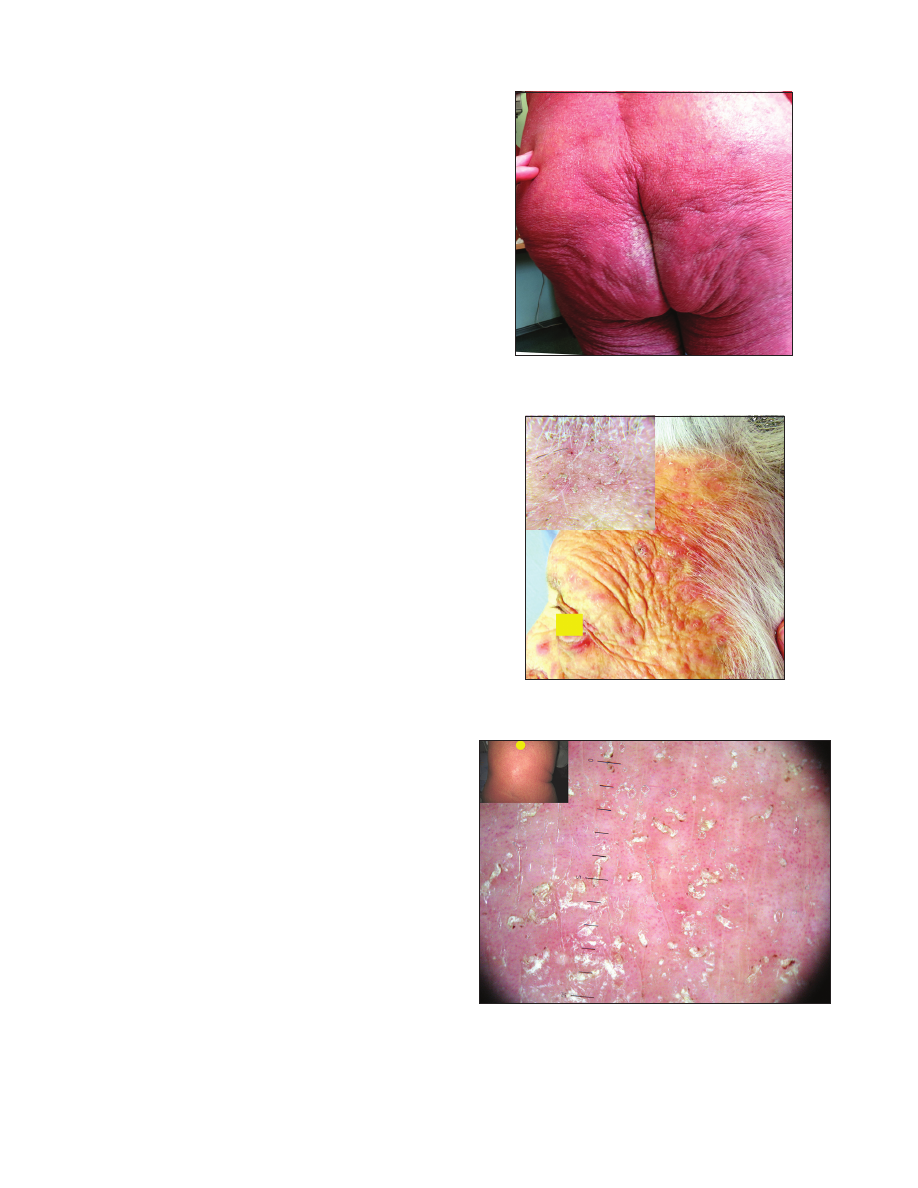
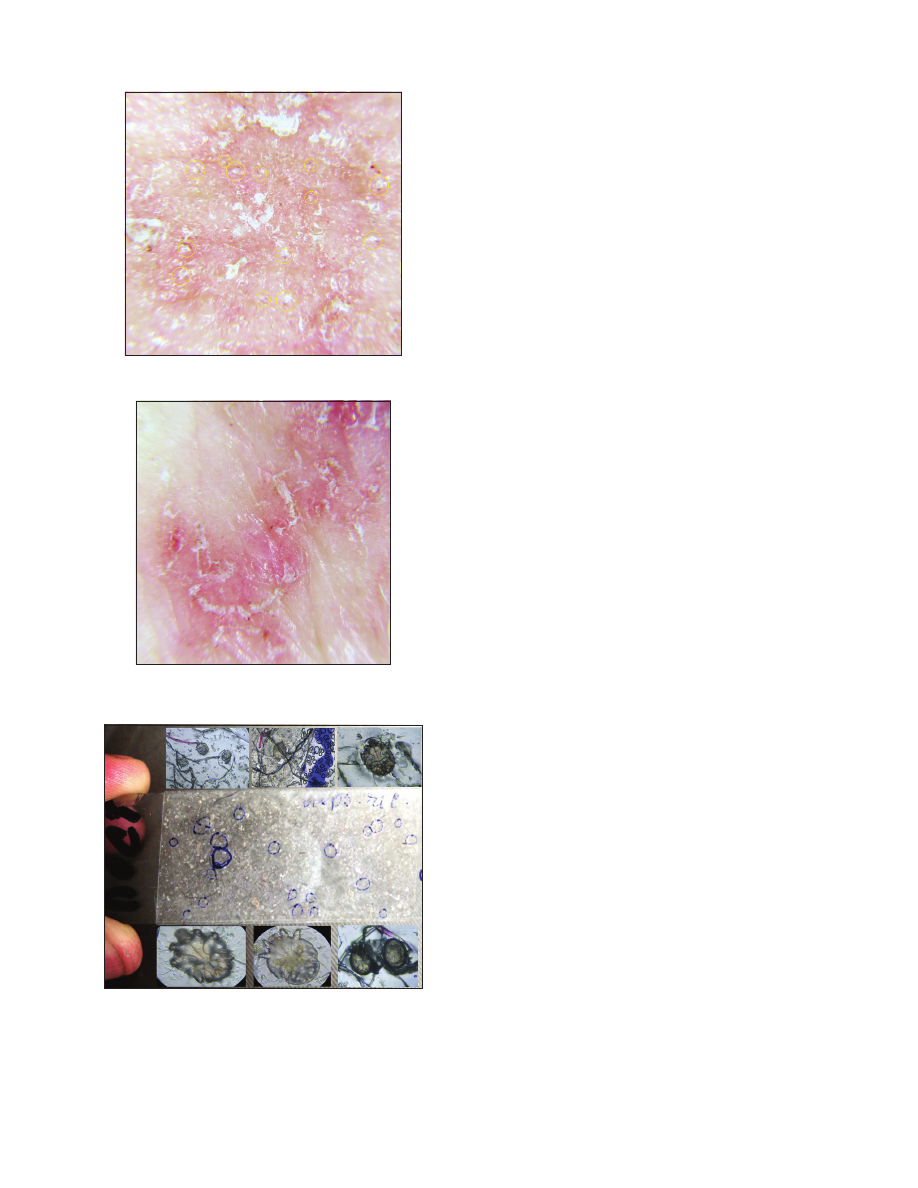
Figure 4:
Mites outside the mite burrows in scabious erythroderma.
Figure 5:
Mites in the apparently little-changed skin in the middle third
of the shin in scabious erythroderma.
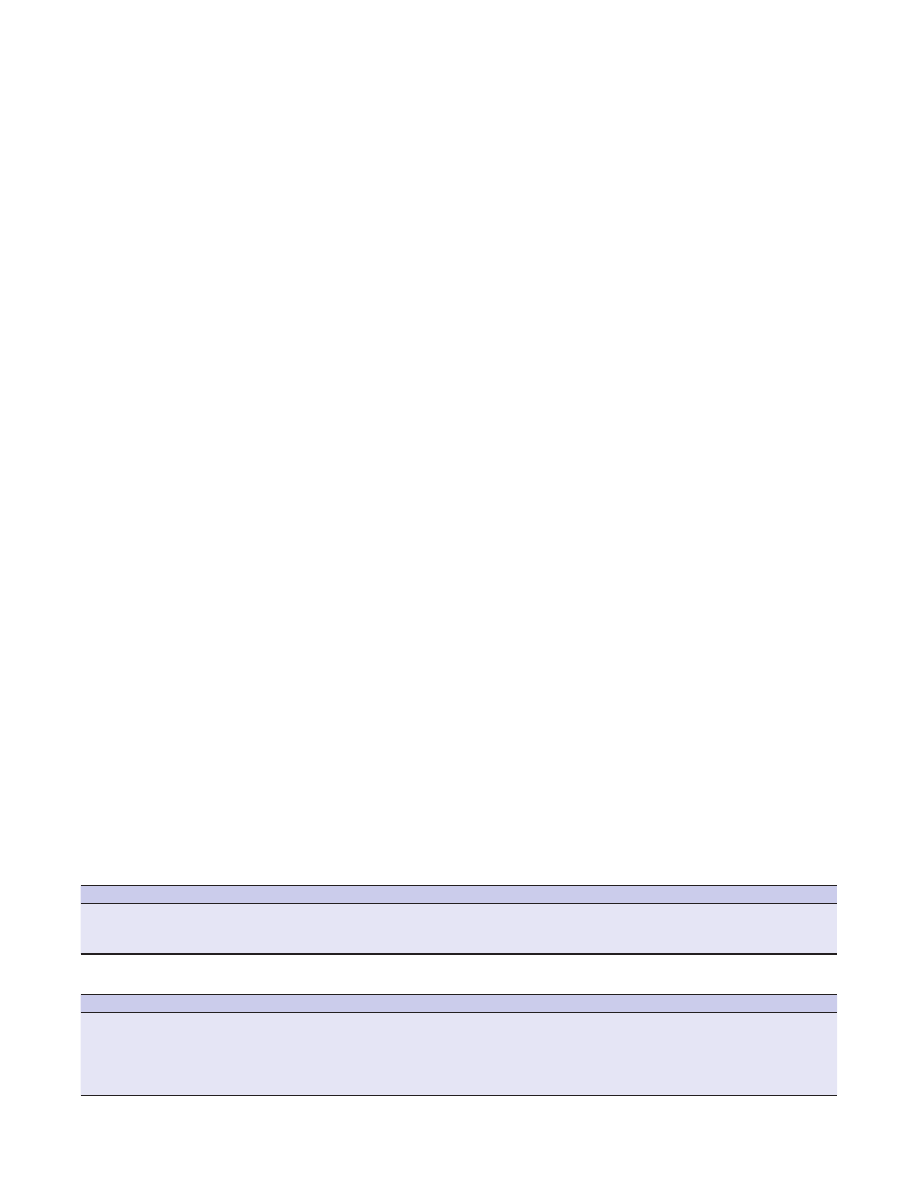
Figure 6:
Scotch test (tape test) from the surface of bed linen: a – slide
with the adhesive tape and visible parasitic elements,
∂ – Parasitic
elements stuck to the tape (eggs, larva).
www.odermatol.com
© Our Dermatol Online 4.2018
359
Dermatoscopy. In all areas of the skin surface multiple
mite burrows were found, including the face, frontal
hairline on the head (Fig. 2), interscapular (Fig. 3) and
pubic (Fig. 4) regions. Mites (from 5 to 30 on 1 cm
2
)
were detected beyond the burrows (Fig. 4) even in only
slightly changed areas (Fig. 5). The number of mites
was the biggest in those areas of the skin surface where
the inflammatory changes were the most dramatic
ones. In order to compare the effectiveness of visual
and dermatoscopic methods for detecting mites, the
parasites were counted on the palm skin surface with
the area of 4 cm
2
. Only female mites located in the
burrows were visually detected (total 19). Twice as many
mites (total 41) were found by means of dermatoscopy,
including parasites beyond the burrows. Microscopy of
skin scrapings yielded the following results (Table 1).
The number of parasitic elements clearly depended on
the size of the skin area to be scraped. In scrapings from
the thigh (6x8 cm) 17 parasitic elements were revealed
and in scrapings from the abdomen the number of
such elements was 25. Adult mites (male and female)
prevailed (40,5%), eggs made up 33,3% of all parasitic
elements, empty egg shells and larvae accounted for
19,1% and 7,1% of elements, respectively. The obtained
data show a high level of mite colonization in those
areas of the skin surface which are only insignificantly
affected in case of common scabies. The prevalence
of female mites and empty egg shells in skin scrapings
speaks for the presence of such burrows which, in case
of common scabies, are usually found on the hands,
wrists and feet.
For the diagnosis of scabies tape-tests were used. Their
results are given in Table 2.
By means of tape-tests taken from 4 sites of the skin
surface 15 mites in various stages of development were
found. The adult mites (imago) dominated including
6 female and 3 male mites. Larvae (6) and nymphs (1)
were also detected, but there were no eggs or egg shells.
Mites were found not only in sites of typical burrow
localization (feet) but also in those areas of the skin
surface where, in case of common scabies, elements
of metamorphic stage of the life cycle are localized
(abdomen, thigh, chest).
While comparing the effectiveness of dermatoscopy
and tape-test methods a considerable advantage of
dermatoscopy was evident. The number of mites
revealed in 4 tape-tests on the area of 10 cm
2
varied
from 2 to 6 parasites. Dermatoscopy of the site with
the same area revealed 35 mites on the foot, 12 on
the abdomen, 22 and 15 on the thigh and chest,
respectively.
Three tape-tests were made with the sheet on which the
patient was lying (Fig. 6 a, b) which revealed 9 female
mites, 6 male mites, 11 larvae, 1 nymph and 4 eggs.
These results speak for a high invasive potential of this
scabies form. All family members who cared for the
patient also had scabies.
With regard to clinical, dermatoscopic and microscopic
data the diagnosis of scabies in the form of scabious
erythroderma was made. The patient was treated
with benzyl benzoate ointment 20%. The next day
the efficacy of the treatment was assessed in terms of
mobility of parasites. Mobility was observed in 67%
of mites extracted from the burrows and in 92% of
mites removed from the apparently normal skin. In
tape-tests taken from the patient’s sheet 23 mites of
27 (85,2%) retained their mobility. Benzyl benzoate
ointment was applied on the whole skin surface
once a day in the evening for 7 days. Simultaneously,
loratadine was administered. On day 8 a significant
reduction of infiltration and hyperemia was observed
and the number of mites on dermatoscopy decreased
Table 1:
Parasitic elements in epidermal scrapings
Site of scrapings
Female mites
Male mites
Larvae
Nymphs
Eggs
Egg shells
Total
Scraping from the thigh (6Χ8 cm)
6
6
0
0
3
2
17
Scraping from the abdomen (20Χ10 cm)
4
1
3
0
11
6
25
Total
10
7
3
0
14
8
42
Table 2:
Parasitic elements in tape-tests taken in various areas of the skin surface
Site of scrapings
Femalemites
Male mites
Larvae
Nymphs
Eggs
Egg shells
Total
Foot
1
3
2
0
0
0
6
Abdomen
0
0
2
0
0
0
2
Thigh
4
0
0
0
0
0
4
Chest
1
0
1
1
0
0
5
Total
6
3
5
1
0
0
15