ВУЗ: Не указан
Категория: Не указан
Дисциплина: Не указана
Добавлен: 02.10.2020
Просмотров: 1293
Скачиваний: 6

©2002 CRC Press LLC
specifically associated with QT
C
interval prolong-
ation bind specifically to the I(kr)
42
.
Although there is little consensus as to what
represents a ‘normal’ QT
C
it is generally accepted
that a QT
C
of over 500 ms increases the likelihood
of an arrhythmia. When interpreting data on
medication-related QT
C
prlongation it is impor-
tant to note that the mean daily QT
C
intrasubject
variability is 76ms
43
.
Other risks factors which increase the
likelihood of QT
C
prolongation include age over
65 years and co-administration of other drugs
associated with cardiac arrythmias, such as tricyc-
lic antidepressants. Safety studies are ongoing with
both the newer and the older medications, prelim-
inary data suggests that the newer medications do
not differ significantly in their likelihood to
prolong the QT
C
interval.
THE NEWER ‘ATYPICAL’ ANTIPSYCHOTICS
The reintroduction of clozapine in the early 1990s
and the subsequent release of several new,
‘atypical’ antipsychotics has increased optimism in
the treatment of schizophrenia. As these are likely
to be the mainstay of treatment for schizophrenia
in the future, it is worthwhile considering them
individually (
Figure 4.17
and
Table 4.3
)
44,45
.
Clozapine
Clozapine,
the prototypical third-generation
antipsychotic, has been used since the 1960s for
treatment of schizophrenia. However, after
reports of several deaths from neutropenia, in
most countries clozapine can be used only in
patients unresponsive to two other antipsychotics
given at an adequate dose for an adequate dura-
tion, or those with tardive dyskinesia or severe
extrapyramidal symptoms, and only with blood
monitoring. Each patient has to be registered and
the drug is dispensed only after a normal white
cell count. In the UK, a blood count is performed
every week for 18 weeks, then every 2 weeks for
the next year, and thereafter monthly. In the USA,
blood monitoring is weekly throughout treatment.
Clozapine is contraindicated for those with
previous neutropenia.
Important aspects of clozapine’s pharmacology
include its low affinity for the D
2
receptor, in
comparison with older antipsychotics. Clozapine
has higher affinity at the D
1
and D
4
receptors than
at the D
2
receptor and also binds to the extra-
striatal D
2
-like receptor, the D
3
receptor. It is
thought that the low incidence of extrapyramidal
side-effects is due to the low activity at the D
2
receptor. Clozapine also has antagonistic activity
at the 5HT
1A
, 5HT
2A
, 5HT
2C
and 5HT
3
Table 4.3 Amisulpride
vs.
reference antipsychotics – selectivity for recombinant human D
2
/D
3
receptor subtypes.
Amisulpride only has appreciable affinity for D
2
and D
3
receptors in contrast to the other antipsychotics in this table.
It has relatively high affinity for both receptors. The implications of this for amisulpride’s mechanism of action and
atypicality are hypothesized to involve an increased tendency to bind to presynaptic D
2
and D
2
-like receptors. Table
reproduced with permission from Schoemaker H, Claustre Y. Fage D,
et al.
Neurochemical characteristics of
amisulpride, an atypical dopamine D
2
/D
3
receptor antagonist with both presynaptic and limbic selectivity.
J
Pharmacol Exp Ther
1997;280:83–97
Positively coupled with
adenyl cyclase
Negatively coupled with adenyl cyclase
Compound
D
1
D
5
D
2
D
3
D
4
Amisulpride
>10000
>10000
2.8
3.2
>1000
Haloperidol
27
48
0.6
3.8
3.8
Clozapine
141
250
80
230
89
Olanzapine
250
–
17
44
–
Risperidone
620
–
3.3
13
–
©2002 CRC Press LLC
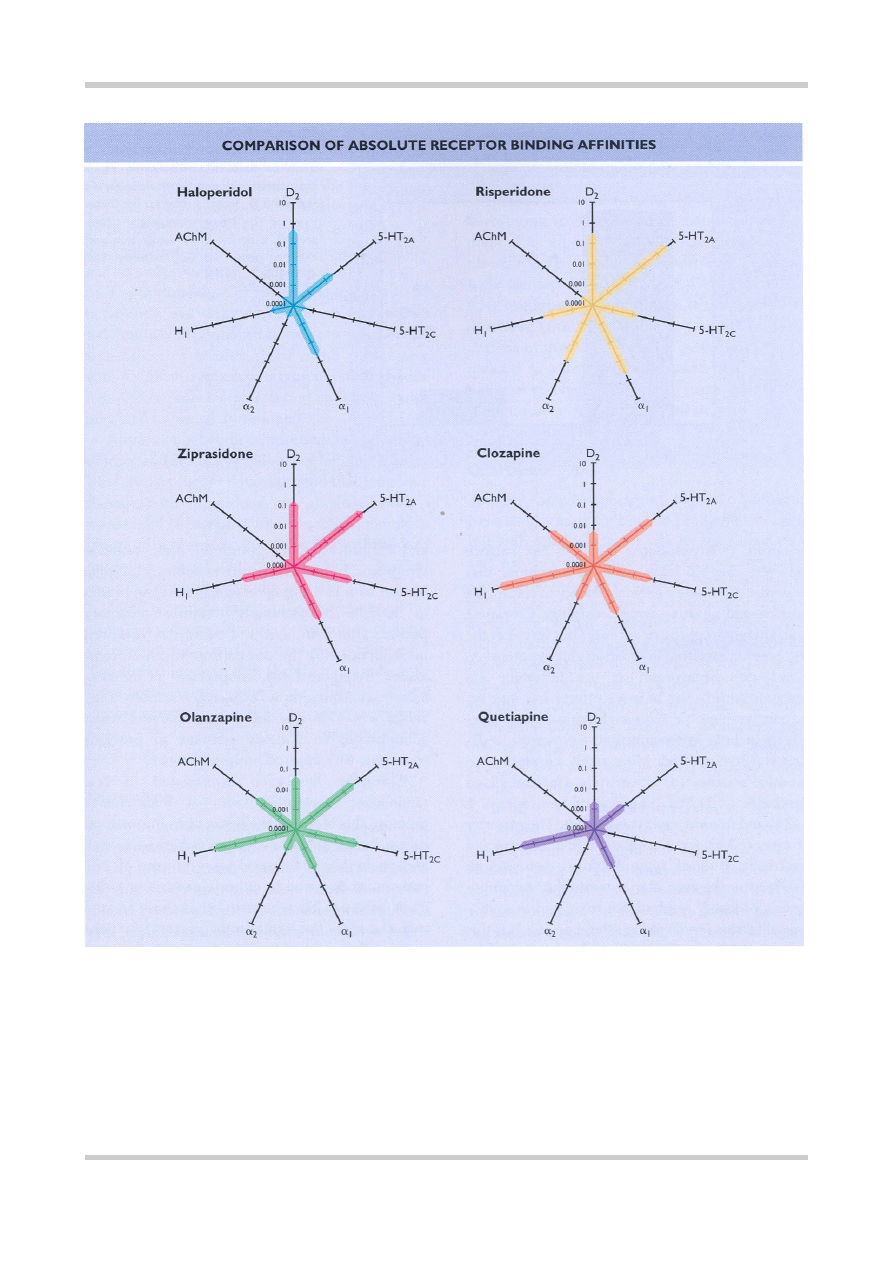
Figure 4.17
A representation of the absolute receptor affinity of haloperidol in comparison with some of the newer ‘atypical’
antipsychotics drawn from data in reference 112. Each line represents a single receptor, the further along the bar on a given line the
higher the affinity of that medication for that receptor. Each of the gradations on the lines represents 10 times greater affinity for that
receptor. What can be seen from this is that clozapine, quetiapine and to a lesser extent olanzapine have much lower affinities for the
dopamine D
2
receptor than haloperidol. This may be why they are ‘atypical’ in terms of producing fewer extrapyrimidal side-effects
than antipsychotics such as haloperidol. Risperidone and ziprasidone have similar D
2
receptor affinities to haloperidol and yet they
too are ‘atypical’. It has been hypothesized that very high affinity for the serotonin-2A receptor, (5-HT
2A
), may underlie the atypicality
of ziprasidone and risperidone. Indeed this may be important for ‘atypicality’
per se
, as all of the newer medications have a higher
affinity for the 5-HT
2A
than for the D
2
receptor. Amisulpride, by contrast to the medications in this figure, only has appreciable affinity
for D
2
and D
3
receptors and has high equipotent affinity for both receptors, as can be seen in
Table 4.3
. Data from reference 45

©2002 CRC Press LLC
receptors. It is postulated that it is the balance
between the blockade of these receptors that
underlies clozapine’s clinical efficacy in improving
positive and negative symptomatology. Clozapine
is an antagonist at the
α
1
receptor but less so at the
α
2
receptor, resulting in sedation and hypotension.
Clozapine’s antagonism at the histamine H
1
receptor adds to the sedative effects and may be,
in part, responsible for weight gain. Other side-
effects include hypersalivation, tachycardia, seda-
tion and hypotension. More rarely, clozapine can
produce seizures (approximately 1%) and blood
dyscrasias (< 1–2%). The risk of neutropenia is
1–2%, and in most cases is reversible. The majority
of cases (83%) occur within the first 20 weeks of
treatment. Risk of agranulocytosis decreases to
0.07% after the first year of treatment. Agranulo-
cytosis probably results from toxic and immuno-
logical factors (reviewed in reference 46). It is this
last potentially fatal side-effect that has led to the
limits on the use of clozapine and the requirement
for blood monitoring in patients receiving cloza-
pine. Interestingly, clozapine does not increase
serum prolactin.
Clozapine is the most effective treatment for
schizophrenic patients refractory to other therapies,
and improves both positive and negative
symptoms. In non-comparative studies, clozapine
has led to > 15% improvement in baseline ratings
in 30–70% of previously treatment-refractory
patients after 2–6 months of treatment (reviewed
in reference 46). In comparison to chlorprom-
azine
47–49
(
Figure 4.18
), haloperidol
50
or fluphen-
azine
51
, clozapine shows a 30–100% response rate,
versus a 4–17% rate for the comparator, when
administered to patients resistant to previous
treatment with classical antipsychotics.
Clozapine has been investigated in few
randomized controlled trials of maintenance
therapy. This is due to the restrictions imposed on
its use. In one of the few studies published, Essock
and co-workers
52
followed up a sample of 227
patients randomized to either clozapine or treat-
ment as usual. They reported that those treated
with clozapine had significantly greater reductions
in side-effects, disruptiveness, hospitalization and
readmission after discharge. Furthermore, the
clinical efficacy of clozapine in relapse prevention
is well established, naturalistically, at 1–2 years of
treatment and there have been reports of good
maintenance efficacy for up to 17 years of
treatment (for review see reference 46).
30%
25%
5%
10%
15%
20%
0%
CLOZAPINE vs. CHLORPROMAZINE IN
TREATMENT-RESISTANT SCHIZOPHRENIA
Clozapine Chlorpromazine
P
roportion of Patients Responding
Figure 4.18
Comparison of efficacy of
clozapine versus chlorpromazine in
treatment-resistant schizophrenia.
Figure reproduced with permission from
Kane J, Honigfeld G, Singer J, Meltzer
H. Clozapine for the treatment-resistant
schizophrenic: a double blind
comparison with chlorpromazine.
Arch
Gen Psychiatry
1988; 45:789–96

©2002 CRC Press LLC
Risperidone
This drug has high affinity for the 5-HT
2A
receptor, with a similar affinity at the D
2
receptor
to most typical antipsychotics. In the acute phase
of treatment, risperidone appears as effective as
haloperidol in terms of improvement in positive
and secondary negative symptom scores
53
.
The optimal dose of risperidone appears to be
between 4 and 6 mg/day. At doses higher than
8–12mg/day risperidone can cause extrapyramidal
side-effects of tremor, rigidity and restlessness,
with a similar frequency to typical antipsychotics.
Risperidone can increase serum prolactin which
may lead to sexual dysfunction.
Risperidone has been assessed for long-term
efficacy and safety in a number of long-term open-
label studies. Earlier data suggested that long-term
therapy with risperidone was associated with a
meaningful reduction in psychopathology, amelio-
ration of extrapyrimidal side-effects (EPS) and
improved social functioning from baseline
measures or against placebo.
More recently a meta-analysis of eleven of the
risperidone/conventional antipsychotic compara-
tor randomized controlled trials was performed
54
.
The author reported that slightly but significantly
more patients on risperidone showed clinical
improvement than with comparison antipsych-
otics (57% vs. 52%) and used significantly less
medication for EPS (29.1% vs. 33.9%).
Olanzapine
A more broad-spectrum atypical antipsychotic,
olanzapine has a side-effect profile similar to that
of clozapine but with a higher incidence of extra-
pyrimidal side-effects at doses above 20 mg/day.
Olanzapine also demonstrates antagonistic effects
at a wide range of receptors, but has a higher
affinity for D
2
and 5-HT
2A
receptors than
clozapine and a lower affinity at the D
1
receptor
subtype. In acute-phase studies, olanzapine is effi-
cacious for positive and secondary negative symp-
toms and was superior to haloperidol on overall
improvement according to the Brief Psychiatric
Rating Scale (BPRS)
55
and every other secondary
measure.
Standard-dose olanzapine (5–15 mg/day) has
been shown to be an effective maintenance treat-
ment for schizophrenia in comparison with
placebo
56
. The estimated 1-year risk of relapse
with olanzapine was 19.6–28.6% for standard-
dose olanzapine in comparison with a 69.9% risk
of relapse with placebo. Initial data from a meta-
analysis of three studies using haloperidol-treated
patients as a test group, indicated that 80.3% of
patients receiving olanzapine maintained their
response at 1 year in comparison with 72% for
haloperidol-treated patients
57
.
Quetiapine
Another broader-spectrum atypical, quetiapine
has a similar receptor binding profile to clozapine,
but with relatively lower affinity for all receptors
and virtually no affinity for muscarinic receptors.
Quetiapine is effective in acute phase studies for
the treatment of positive and secondary negative
symptoms. Initial randomized controlled trials
indicated that quetiapine (250–750mg, n=96) was
more effective than placebo (n = 96) and that this
efficacy was not seen at doses of less than 250
mg/day of quetiapine
58
. In comparison with chlor-
promazine, response rates to quetiapine were
similar across all symptom domains
59
. Response
rates between haloperidol- and quetiapine-treated
groups are also similar
60
.
In all of these studies, the rates of EPS with
quetiapine were similar to those seen in placebo-
treated groups and significantly lower than in conv-
entional antipsychotic comparator groups. Most
common side-effects are somnolence and dry
mouth. Quetiapine demonstrates a lower potential
to cause weight gain than clozapine and olanzapine,
and does not increase serum prolactin
61
.
In long-term studies, quetiapine was well
tolerated with up to 75% of respondents to a
questionnaire denying any side-effects from
quetiapine
62
.
©2002 CRC Press LLC
Amisulpride
In contrast to all the other newer antipsychotics,
amisulpride only has effects on the dopamine D
2
and D
3
receptors, where it is a potent antagonist.
In animal models at lower doses, amisulpride
appears to bind preferentially to presynaptic D
2
receptors
64
, and at projected therapeutic levels it
also appears to be selective, in a neurochemical
imaging study in humans, for limbic D
2
and D
3
receptors
63
. It has a similar efficacy to haloperidol
for positive symptoms in acute exacerbations of
schizophrenia
64–67
, with a projected optimum
dose in this group of between 400 and 800
mg/day
66
. Some studies at this dose range have
reported a significantly greater efficacy for amisul-
pride in comparison with placebo for treating the
negative symptoms of schizophrenia
65,66
.
In all of the studies above, amisulpride has a
significantly lower incidence of extrapyrimidal
side-effects, at doses below 1200 mg/day, than
haloperidol. Amisulpride may cause less weight
gain than other atypical antipsychotics but it does
increase plasma prolactin
68,69
.
In a 12-month trial of amisulpride
200–800 mg/day versus haloperidol 5–20 mg/day,
amisulpride showed enhanced efficacy for positive
and negative symptoms in comparison with halo-
peridol. Those treated with amisulpride had
significantly greater improvement in quality of life
and significantly fewer extrapyrimidal side-effects.
Long-term efficacy and relapse prevention were
similar in the amisulpride- and haloperidol-treated
groups
70
.
Ziprasidone
Ziprasidone has a high 5HT
2A
/D
2
receptor
blockade ratio and a similarly high affinity for the
5HT
2A
receptor to risperidone and sertindole. It is
an agonist at the 5HT
1A
receptor. Ziprasidone also
has potent affinity for D
3
and moderate affinity
for D
4
receptors. It exhibits weak serotonin and
noradrenergic reuptake inhibition.
Ziprasidone appears to have relatively low
levels of side-effects. These may include somno-
lence and headache, but results of full clinical
studies remain to be published.
An initial clinical trial of ziprasidone versus
haloperidol 15 mg/day over 4 weeks suggested
that ziprasidone 160 mg/day was as effective as
haloperidol at reducing positive symptom scores,
but produced fewer side-effects
71
. In two placebo-
controlled trials lasting 4 and 6 weeks,
respectively
72,73
, the pooled data indicated that
ziprasidone 80–160 mg was consistently signi-
ficantly more effective than placebo and lower
doses of ziprasidone. Improvements in positive
and negative symptoms were similar in magnitude
to those seen in patients treated with risperidone,
olanzapine or quetiapine. Interestingly, 160 mg of
ziprasidone was associated with a greater than
30% decrease in depressive symptoms in the sub-
group of patients with significant depression at the
outset of the trials.
Ziprasidone has also been used in a 1-year
placebo-controlled trial in order to assess its utility
for relapse prevention. A total of 294 patients
were studied and randomized to placebo treat-
ment or ziprasidone 40–160 mg/day. At 6 months
into the study, 117 patients remained on
ziprasidone and 23 on placebo. Of these, only 6%
of the ziprasidone-treated patients had experien-
ced an exacerbation of their symptoms over the
subsequent 6 months, in comparison with 35% in
the placebo-treated group
74
.
NEW ANTIPSYCHOTICS CURRENTLY IN
PHASE III CLINICAL TRIALS
Iloperidone
Iloperidone is a benzisoxazole derivative and is
therefore from the same chemical class as
risperidone. As for risperidone, iloperidone has a
high affinity for the 5-HT
2A
receptor and a lower
affinity for the D
2
receptor, although in absolute
terms its affinity for the D
2
receptor is of a similar
order of magnitude to haloperidol and risperidone.
Relative to other newer antipsychotics iloperidone
has a higher affinity for 5-HT
1A
receptors and
lower affinity for 5-HT
2C
receptors
75
. It also has
high affinity for
a
1
receptors but no affinity for
acetylcholine muscarinic M
1
receptors.