ВУЗ: Не указан
Категория: Не указан
Дисциплина: Не указана
Добавлен: 02.10.2020
Просмотров: 1296
Скачиваний: 6
©2002 CRC Press LLC
matched healthy controls
13,14
. Previous studies
with PET and SPET have indicated that the
‘atypical’ and newer antipsychotic medications
like clozapine, risperidone, olanzapine and sertin-
dole all lead to almost complete occupancy of
cortical 5-HT
2A
receptors at clinically relevant
doses
15–17
(
Figure 4.9
) Full characterization of the
effects of the older typical antipsychotics on
5-HT
2A
receptors remains to be completed,
however, preliminary data indicates that broad-
spectrum typical antipsychotics such as pheno-
thiazines and thioxanthines also lead to a
significant occupancy (or reduction in receptor
availability) of cortical 5-HT
2A
receptors, but the
level of occupancy is still significantly lower than
that seen with the newer medications
18
.
There is a neuroanatomical and functional
interaction of 5-HT and dopaminergic systems
such that blocking 5-HT
2A
receptors enhances
dopaminergic transmission. The newer atypical
antipsychotics, in contrast with the typical anti-
psychotics, all have a higher affinity for the
5-HT
2A
receptor than for the D
2
receptor. In
terms of treatment response, there is a correlation
of serotonergic neuroendocrine responses with
symptomatic improvement on clozapine and
preliminary data suggesting that allelic variations
in the 5-HT
2A
receptor gene vary with, and may
predict, treatment response
10
.
PET studies of 5-HT
2A
receptor density in
drug-naive patients with schizophrenia have failed
to show any difference in comparison with
255
248
208
180
127
102
94
Temporal
cortex and
cerebellum
Frontal,
parietal and
occipital
cortices
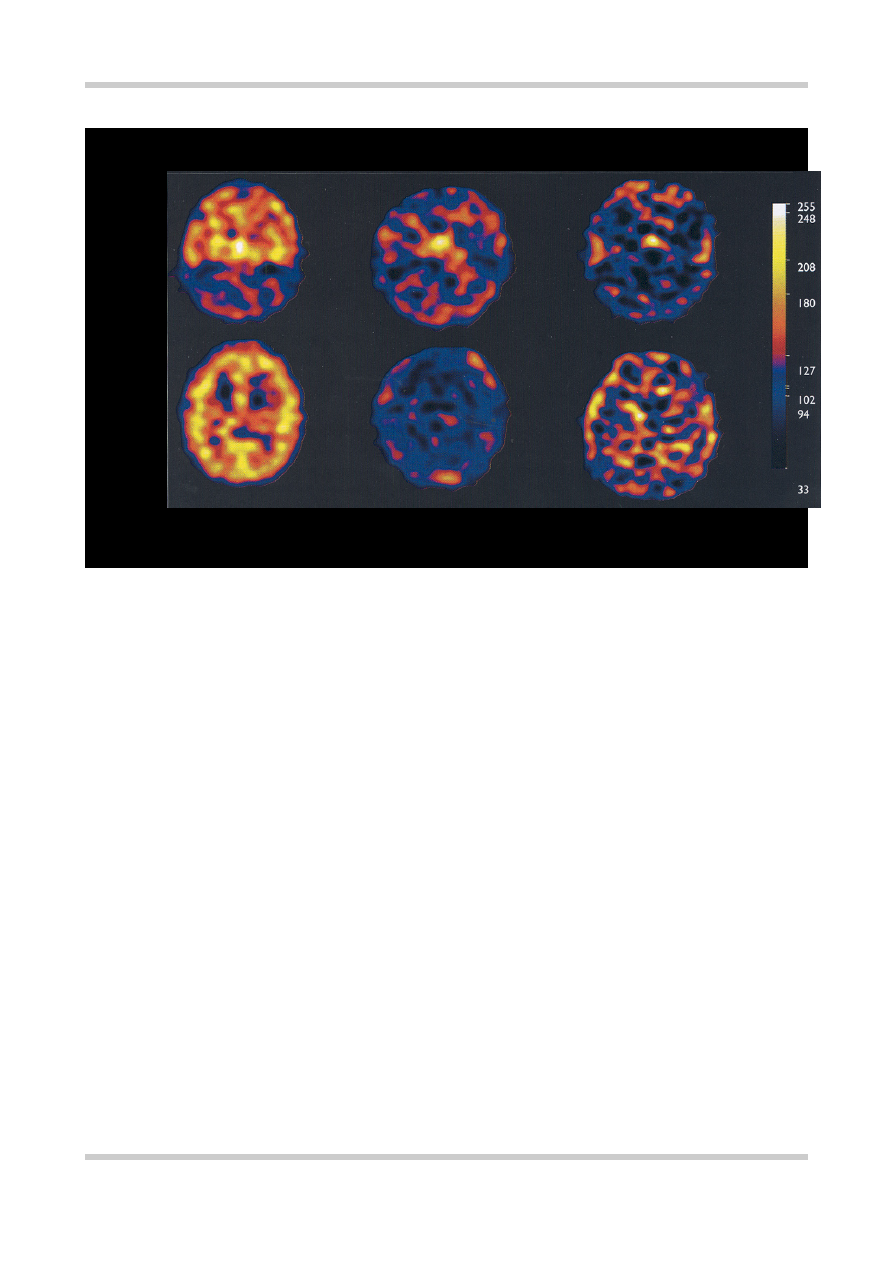
SPET SCANS OF 5-HT
2A
RECEPTOR DENSITY
Healthy volunteer Clozapine treated Risperidone treated
Figure 4.9
Single photon emission tomography (SPET) scans of 5-HT
2A
receptor density in a healthy volunteer and two
patients with schizophrenia receiving a therapeutic dose of either clozapine (450 mg/day) or risperidone (6 mg/day). In the
slice at the level of the frontal, parietal and occipital cortices from the healthy volunteer the ubiquitous distribution of 5-HT
2A
receptors in the cortical gray matter can be seen. This binding of the tracer is absent from the equivalent slices from the
medicated patients. This indicates that both clozapine and risperidone are producing very high or ‘saturation’ levels of 5-
HT
2A
receptor blockade. This high level of blockade may confer some protection against the development of EPS and may
be one of the mechanisms of antipsychotic ‘atypicality’. Figure reproduced with permission from Travis MJ, Busatto GF,
Pilowsky LS,
et al.
5-HT
2A
receptor blockade in patients with schizophrenia treated with risperidone or clozapine. A SPET
study using the novel 5-HT
2A
ligand 123I-5-I-R-91150.
Br J Psychiatry
1998;173:236–41

©2002 CRC Press LLC
More than nine distinct serotonin (5-HT)
receptors have been identified. The 5-HT
1A
, 5-
HT
2A
, 5-HT
2C
, and 5-HT
3
receptors have been
most extensively studied. The major site of
serotonergic cell bodies is in the area of the upper
pons and midbrain. The classic areas for 5-HT-
containing neurons are the median and dorsal
raphe nuclei. The neurons from the raphe nuclei
project to the basal ganglia and various parts of the
limbic system, and have a wide distribution
throughout the cerebral cortices in addition to
cerebellar connections (
Figure 4.10
). All the 5-HT
receptors identified to date are G-protein coupled
receptors, except the 5-HT
3
receptor, which is a
ligand gated Na
+
/K
+
channel.
5-HT is synthesized from tryptophan by
tryptophan hydroxylase, and the supply of
tryptophan is the rate-limiting step in the
Figure 4.10
Representation of the primary serotonin-containing tracts in the human brain. Arising from the raphe
nuclei these cells project to all cortical gray matter, with additional tracts to the basal ganglia and the cerebellum
SEROTONINERGIC PATHWAYS
A Caudal raphe nuclei
B Rostral raphe nuclei
C Deep cerebellar nuclei
D Limbic structures
E Thalamus
F Neocortex
G Cingulum
H Cingulate gyrus
I To hippocampus
C
E
F
H
I
D
A
B
G

©2002 CRC Press LLC
synthesis of 5-HT (
Figure 4.11
). 5-HT is primarily
broken down by monoamine oxidase and the
primary metabolite is 5-HIAA.
Other neurotransmitters
Recent efforts have been directed towards finding
an alternative neurochemical target in schizo-
phrenia. The first of these that should be
considered is gamma aminobutyric acid (GABA).
GABA appears to have a regulatory role on dopa-
minergic function. The balance of evidence tends
to suggest that GABA decreases dopaminergic
firing. This links with human postmortem data
indicating that GABAergic reductions correlate
with increased dopamine concentrations
19,20
.
Thus, it is possible that in schizophrenia there is a
reduction in GABAergic function which leads to a
dysregulation of dopamine and the production of
psychotic symptoms. A more likely candidate,
however, appears to be the glutamatergic system.
Glutamatergic dysfunction, particularly at the
level of the N-methyl-D-aspartate (NMDA)
receptor, has also been implicated in the patho-
physiology of schizophrenia. Drugs which are
antagonistic at the NMDA receptor, such as
ketamine and phencyclidine, produce in healthy
volunteers, both the positive, negative and
neurocognitive symptoms that are characteristic
of schizophrenia
21
. There is evidence that the pro-
psychotic effects of these drugs may be mediated
via an increase in the release of glutamate acting
on non-NMDA receptors
22
.
If the function of NMDA receptors themselves
is decreased this may remove the glutamatergic
Figure 4.11
The rate-limiting
step for serotonin synthesis is
the availability of the precursor
tryptophan. Tryptophan
hydroxylase is the rate limiting
enzyme. Serotonin in the CNS
is primarily metabolized by
monoamine oxidase. The
primary metabolite is 5-
hydroxyindoleacetic acid
Tryptophan
5-Hydroxytryptophan
L-aromatic
acid decarboxylase
Tryptophan
hydroxylase
Monoamine
oxidase
Aldehyde
dehydrogenase
Serotonin (5-HT)
5-Hydroxyindoleacetic
acid (5-HIAA)
N
H
NH
2
COOH
CH
2
CH
HO
SEROTONIN SYNTHESIS AND METABOLISM
N
H
NH
2
COOH
CH
2
CH
HO
N
H
CH
2
CH2NH2
HO
N
H
CH
2
CHO
HO
N
H
CH
2
COOH

©2002 CRC Press LLC
drive to inhibitory GABAergic neurons which
further regulate the excitatory neurons acting on
areas such as the frontal cortex and the limbic
regions. Thus, with decreased inhibitory control
these neurons may increase firing in these areas
and produce psychotic symptoms
23
. Thus, redu-
cing glutamate release at all glutamate receptors
may also have a role in improving symptoms in
schizophrenia.
EFFICACY OF ANTIPSYCHOTICS IN THE
ACUTE PHASE OF TREATMENT
The best known large-scale clinical trial, which
gives a good idea of the treatment effect to be
expected with antipsychotics, was carried out by
the National Institutes of Mental Health, in the
USA
24
. This study involved four treatment groups
(chlorpromazine, thioridazine, fluphenazine and
placebo) with 90 randomly allocated subjects in
each. The subjects were treated for 6 weeks and
rated on 14 different symptoms in addition to
global clinical improvement. In this study 75% of
subjects in the chlorpromazine, thioridazine and
fluphenazine groups showed significant improve-
ment, 5% failed to be helped and 2% deteriorated.
In the placebo group only 25% of patients showed
significant improvement, and over 50% were
unchanged or worse.
Johnstone and co-workers
25
, showed that
pimozide was antipsychotic (i.e. reducing the
positive symptoms of psychosis) in patients with
‘functional’ psychosis, regardless of whether the
patients had prominent manic or depressive symp-
toms or were euthymic. This proved that ‘neuro-
leptics’, as they were then popularly called, were
truly antipsychotic rather than simply antischizo-
phrenic (
Figure 4.12
).
Figure 4.12
Change in positive psychotic symptoms in patients randomized to either the antipsychotic
pimozide or to placebo. The groups were subdivided on the basis of the presence of elevated mood,
depressed mood or no consistent mood change. The fact that pimozide significantly reduced positive
psychotic symptoms in all three groups provided evidence that the ‘neuroleptics’ are in fact antipsychotic
rather than ‘antischizophrenic’. Figure reproduced with permission from Johnstone EC, Crow TJ, Frith
CD, Owens DG. The Northwick Park “functional” psychosis study: diagnosis and treatment response.
Lancet
1988;2:119–25
100
20
40
60
80
0
Pe
rcentage change
Elevated mood
Time (weeks)
0
1
2
3
4
0
1
2
3
4
0
1
2
3
4
Placebo (a)
Pimozide (b)
a vs. b
p
< 0.05
a vs. b
p
< 0.01
a vs. b
p
< 0.05
Depressed mood No consistant
mood change
PERCENTAGE CHANGE IN POSITIVE PSYCHOTIC SYMPTOMS

©2002 CRC Press LLC
Davis and Andriukaitis
26
performed a meta-
analysis using the trials involving chlorpromazine,
to investigate the relationship between dose and
clinical effect. They noted that a threshold of
400 mg chlorpromazine was required. This was
based on the fact that in 31 trials using a dose of
400 mg chlorpromazine/day, only one trial failed
to show that chlorpromazine was more effective
than the non-antipsychotic reference treatment,
whereas in the 31 trials using a dose < 400 mg of
chlorpromazine, 19 had failed to show a signifi-
cant effect.
No comparative trials have shown a consistent
superiority in any treatment outcome for one
conventional or typical antipsychotic over another
in the acute treatment of schizophrenia
27
.
PHARMACOTHERAPY AS MAINTENANCE
TREATMENT IN SCHIZOPHRENIA
Although it is widely accepted that antipsychotic
medication is the mainstay of treatment in acute
schizophrenia, its role in long-term maintenance
has been more contentious. Nevertheless, the
importance of maintenance drug therapy in the
treatment of chronic schizophrenia has been
evident since the early 1960s.
Initial studies indicated that between one-half
and two-thirds of patients with schizophrenia who
were stable on medication relapsed following
cessation of maintenance pharmacological ther-
apy, compared with between 5 and 30% of the
patients maintained on medication
28–30
.
In a review of 66 studies from 1958 to 1993,
Gilbert and colleagues
31
noted that relapse rate in
the medication withdrawal groups was 53.2%
(follow-up 6.3–9.7 months) compared with
15.6% (follow-up 7.9 months) in the maintenance
groups. There was also a positive relationship
between risk of relapse and length of follow-up.
Viguera and colleagues
32
investigated the relation-
ship between gradual (last depot injection or
tailing off over 3 weeks or more) and abrupt
medication discontinuation. They noted a cumula-
tive relapse rate of about 46% at 6 months and
56.2% at 24 months of follow-up in patients
whose medication was stopped abruptly. They
calculated that in patients whose medication was
Figure 4.13
The upper line
represents the percentage of patients
with schizophrenia who remained
stable after gradual reduction of
antipsychotic medication. The lower
line represents patients whose
medication was abruptly stopped.
These results indicate that abrupt
cessation of antipsychotic medi-
cation produces a much higher risk
of relapse in schizophrenia than a
gradual reduction. Figure
reproduced with permission from
Viguera AC, Baldessarini RJ, Hegarty
JD,
et al
. Clinical risk following
abrupt and gradual withdrawal of
maintenance neuroleptic treatment.
Arch Gen Psychiatry
1997;54:
49–55
100
50
40
60
70
80
90
30
20
Pe
rcentage
remaining stable (%)
Weeks after stopping antipsychotic therapy
16
20 24
12
8
4
0
Gradual (n = 58)
Abrupt (n = 49)
RELAPSE AFTER STOPPING ANTIPSYCHOTICS