ВУЗ: Не указан
Категория: Не указан
Дисциплина: Не указана
Добавлен: 02.10.2020
Просмотров: 2553
Скачиваний: 7

©2002 CRC Press LLC
‘Functional’
Schizotypal disorder
Persistent delusional disorders
Acute and transient psychotic disorders
Schizoaffective disorders
Induced delusional disorder
Mania
Other nonorganic psychotic disorders
‘Organic’
Drug/substance-induced psychosis (e.g.
alcohol withdrawal, amphetamines, crack
cocaine, LSD, cannabis, PCP, and also
steroids, dopamine agonists and some heavy
metals)
Epilepsy – in particular, the fits of temporal
lobe epilepsy may resemble an acute
psychotic episode
Tumors, either primary or secondary
Stroke
Early dementia
Long-term sequelae of head injury
Endocrine causes (e.g. Cushing’s disease;
rarely hyper- and hypothyroidism)
Infections (e.g. encephalitis, meningitis,
neurosyphilis)
Multiple sclerosis
Autoimmune disorders such as systemic
lupus erythematosus (SLE)
Metabolic disorders (e.g. hepatic failure,
uremia, hypercalcemia, acute intermittent
porphyria)
DIFFERENTIAL DIAGNOSIS OF
SCHIZOPHRENIA
Hallucinations are defined as false
perceptions in the absence of a real external
stimulus. They are perceived as having the
same quality as real perceptions and are not
usually subject to conscious manipulation.
Hallucinations in schizophrenia may
involve any of the sensory modalities. The
most common are auditory hallucinations in
the form of voices, which occur in 60–70% of
patients diagnosed with schizophrenia.
Although voices in the second person are
most common, the characteristic
‘Schneiderian’ voices are in the third person
and provide a running commentary on the
patient’s actions, arguing about the patient or
repeating the patient’s thoughts. Voices may
be imperative, ordering the patient to harm
himself or others. Visual hallucinations occur
in about 10% of patients, but should make
one suspicious of an organic disorder.
Olfactory hallucinations are more common in
temporal lobe epilepsy than schizophrenia,
and tactile hallucinations are probably
experienced more frequently than is reported
by patients.
No single type of hallucination is specific
to schizophrenia, and the duration and
intensity are probably most important
diagnostically.
HALLUCINATIONS

©2002 CRC Press LLC
Ambitendence
Alternation between opposite
movements.
Echopraxia
Automatic imitation of another
person’s movements even when asked not to.
Stereotypies
Repeated regular fixed parts of
movement (or speech) that are not goal
directed, e.g. moving the arm backwards and
outwards repeatedly while saying ‘but not for
me’.
Negativism
Motiveless resistance to
instructions and attempts to be moved, or
doing the opposite of what is asked.
Posturing
Adoption of inappropriate or
bizarre bodily posture continuously for a
substantial period of time.
Waxy flexibility
The patient’s limbs can be
‘molded’ into a position and remain fixed for
long periods of time.
CATATONIC SYMPTOMS
These mainly motor symptoms may occur in any form of schizophrenia but are
particularly associated with the catatonic subtype
Usually a disorder of the form of thought,
such that the speech is difficult to follow or
incoherent and follows no logical sequence.
Knight’s move thinking
(or derailment)
occurs when the patient moves from one train
of thought to another which has no apparent
connection to the first – it takes its name from
the chess piece that moves two steps forward
and one to the side. A less severe form is
called
loosening of associations
which
merges into
tangential thinking
and
loss of
goal
.
Some patients may invent
neologisms
(new words), exhibit
verbal stereotypy
(repetition of a single word or phrase out of
context), or use
metonyms
(ordinary words
given a special personal meaning).
Negative thought disorder includes
poverty of speech
(limited quantity of
speech), and poverty of content of speech
(limited meaning conveyed by speech).
THOUGHT DISORDERS
Disorders of thought possession in schizo-
phrenia are sometimes called thought aliena-
tion. The patient has the experience that his
thoughts are under the control of an outside
agency or that others are participating in his
thinking.
Thought insertion
The patient believes that
thoughts that are not his own are being put
into his mind by an external agency.
Thought withdrawal
The patient believes
that thoughts are being removed from his
mind by an external agency.
Thought broadcasting
The patient believes
that his thoughts are being ‘read’ by others, as
if they were being broadcast.
Thought blocking
Involves a sudden
interruption of the train of thought, before it is
completed, leaving a ‘blank’. The patient sud-
denly stops talking and cannot recall what he
has been saying or thinking.
DISORDERS OF THOUGHT POSSESSION


©2002 CRC Press LLC
A delusion is a fixed, false personal belief held
with absolute conviction despite all evidence
to the contrary. The belief is outside the
person’s normal culture or subculture and
dominates their viewpoint and behavior.
Delusions may be described in terms of their
content
(e.g. delusions of persecution or
grandeur). They can be
mood congruent
(the
content of delusion is appropriate to the mood
of the patient), or
mood incongruent
.
Delusions are described as
systematized
if they
are united by a single theme.
A
primary delusion
arises fully formed
without any discernible connection with
previous events (also called autochthonous
delusions), e.g. “I woke up and knew that my
daughter was the spawn of Satan and should
die so that my son could be the new Messiah”.
Secondary delusions
can be understood in
terms of other psychopathology, for example
hallucinations: “The neighbors must have
connected all the telephones in the building;
that’s why I can hear them all the time”.
The term delusional mood is slightly
confusing in that it does not describe an
abnormal belief, but refers to an ill-defined
feeling that something strange and threatening
is happening which may manifest as perplexity,
uncertainty or anxiety. This may precede a
primary delusion or a delusional perception,
which involves a real perception occurring
almost simultaneously with a delusional
misinterpretation of that perception, e.g. “I saw
the traffic lights change from red to green and
knew that I was the rightful heir to the throne of
England”.
Overvalued ideas
are unreasonable and
sustained intense preoccupations maintained
with a strong emotional investment but less
than delusional intensity. The idea or belief
held is demonstrably false and not usually held
by persons from the same subculture.
Delusions may be classified in terms of their
content, for example delusions of...
Persecution
An outside person or force is in
some way interfering with the sufferer’s life or
wishes them harm, e.g. “The people upstairs
are watching me by using satellites and have
poisoned my food”.
Reference
The behavior of others, objects, or
broadcasts on the television and radio have a
special meaning or refer directly to the person,
e.g. “A parcel came from Sun Alliance and the
radio said that ‘the son of man is here’, on a
Sunday, so I am the son of God”.
Control
The sensation of being the passive
recipient of some controlling or interfering
agent that is alien and external. This agent can
control thoughts, feeling and actions (passivity
experiences), e.g. “I feel as if my face is being
pulled upwards and something is making me
laugh when I’m sad”.
Grandeur
Exaggerated belief of one’s own
power or importance, e.g. “I can lift mountains
by moving my hands, I could destroy you!”.
Nihilism
Others, oneself, or the world does not
exist or is about to cease to exist (often called
Cotard’s syndrome), e.g. “The inside of my
tummy has rotted away. I have no bowels”.
Infidelity
One’s partner is being unfaithful
(also known as delusional jealousy or the
Othello syndrome).
Doubles
A person known to the patient, most
frequently their spouse, has been replaced by
another (also known as Capgras’ syndrome or,
confusingly, ‘illusion’ of doubles).
Infatuation
A particular person is in love with
the patient (also known as erotomania or de
Clerambault’s syndrome).
Somatic
Delusional belief pertaining to part of
the person’s body, e.g. “My arms look like
they’ve been melted and squashed into a
mess”.
DELUSIONS

©2002 CRC Press LLC
THE ACUTE ILLNESS
The onset may be rapid, or slow and insidious. In
the latter situation in particular, there may be a
prolonged period of undiagnosed illness in which
the affected person slowly becomes more with-
drawn and introverted. They may develop unusual
interests, particularly of a religious or philo-
sophical kind, and drift away from family and
friends. They may also begin to fail in their
occupation or schoolwork. This process can take
weeks to years but eventually, often with a
seemingly precipitating event, the symptoms of
florid illness appear.
The acute symptoms are variable but usually
include delusions, hallucinations, abnormal
thought processes and passivity experiences
(
Figures 1.11
–
1.16
). In addition, there may be
formal thought disorder, and flat or inappropriate
affect. Abnormal motor signs, sometimes termed
catatonic, used to be common but now are much
less so in Western countries. At this stage of the
illness, positive symptoms tend to dominate the
clinical picture.
Figure 1.11
Castle of Bad Dreams, by Phyllis Jones, 1936. This picture “Served a double purpose, firstly to
illustrate one of Grimm’s fairytales of ‘The foolish old woman’ and her wishes, and secondly to symbolize her
own life”. It is tempting to speculate that it indicates a depressive component to her symptoms. Reproduced
with kind permission of the Bethlem Royal Hospital Archives and Museum, Beckenham, Kent, UK
©2002 CRC Press LLC
Figure 1.13
Puppeteers, by Phyllis Jones, 1936. This
patient was a talented artist, who was admitted to a
psychiatric hospital at the age of 22 years complaining of
hearing voices, and convinced her food was being
poisoned. The clinical description suggests a florid
psychotic illness, of acute onset, accompanied by severe
affective disturbance. Reproduced with kind permission of
the Bethlem Royal Hospital Archives and Museum,
Beckenham, Kent, UK
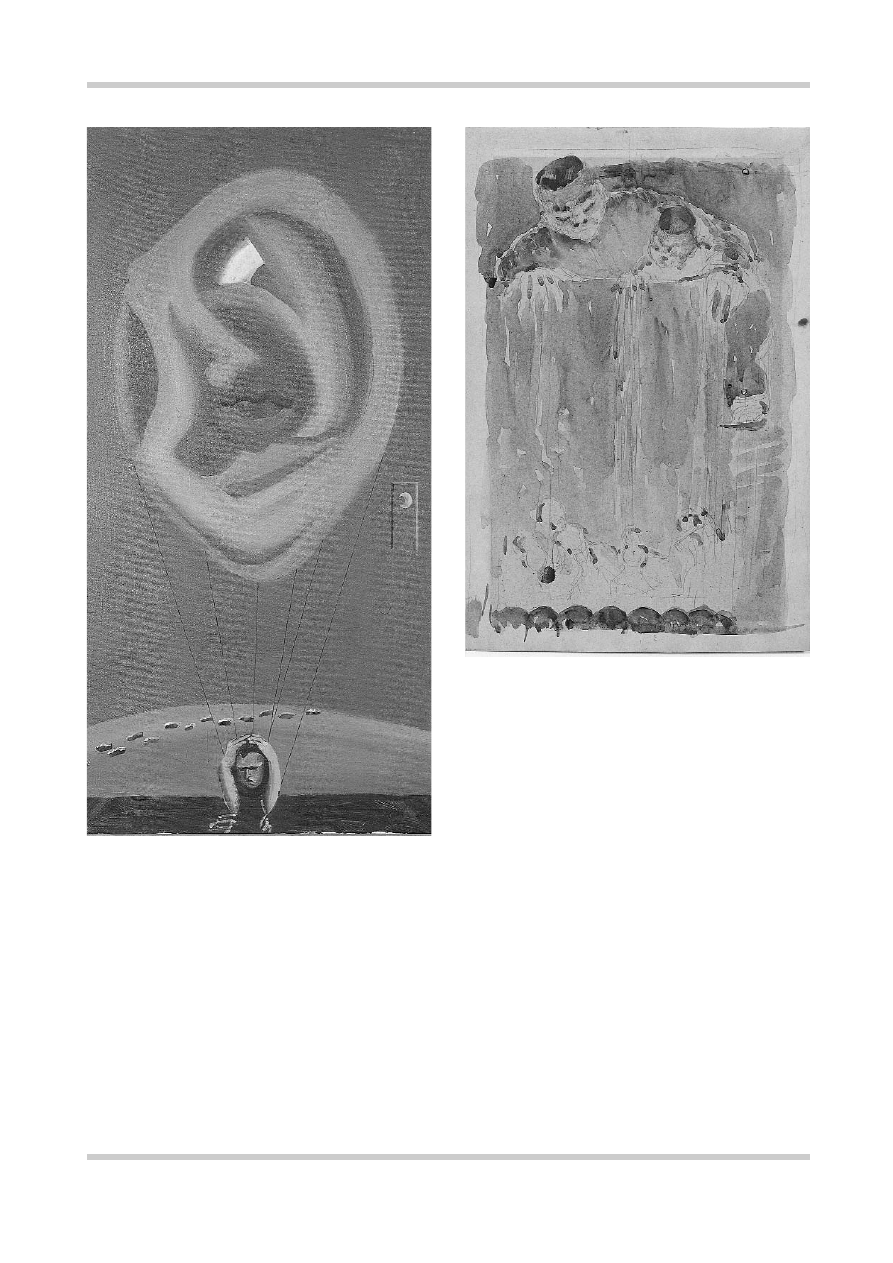
Figure 1.12
Grey self-portrait, by Bryan Charnley. This
painting illustrates aspects of Charnley’s psychotic
symptoms, including that of hearing voices. Reproduced
with kind permission of the Bethlem Royal Hospital
Archives and Museum, Beckenham, Kent, UK