ВУЗ: Не указан
Категория: Не указан
Дисциплина: Не указана
Добавлен: 02.10.2020
Просмотров: 2562
Скачиваний: 7
©2002 CRC Press LLC
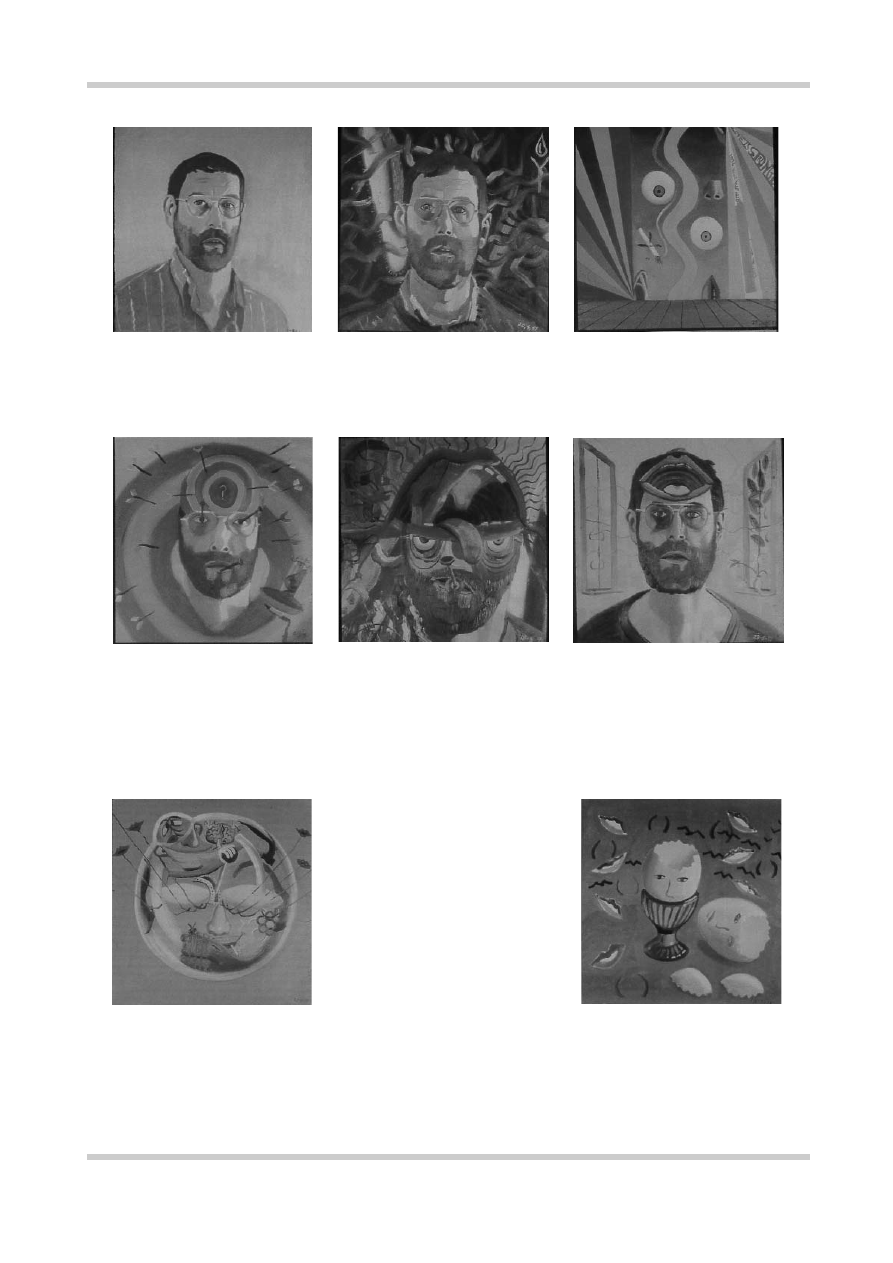
Figure 1.20
A series of self-portraits by Bryan Charnley which vividly illustrate his experiences as he came off
medication. His descent into paranoia, hallucinations and depression is graphically depicted and explained with
reference to his diary entries. Sadly the series ended with his death from suicide. Figures reproduced with kind
permission of Mr Terence Charnley
Self-portrait 11–16 April 1991
April 20: ‘Very paranoid...The person
upstairs is reading my mind and speaking
back to me in a sort of ego crucifixion...The
large rabbit ear is because I am confused
and extremely sensitive to human voices,
like a wild animal.’
May 6: has turned himself into a
dartboard. ‘I feel like a target for people’s
cruel remarks. What is going on? I have
sweet talked a girl to suicide because I
had no tongue, no real tongue and could
only flatter.’
May 23: ‘The blue is there because I feel
depressed, through cutting back on the
antidepressants...the wavy lines are
because just as I feel I am safe, a voice
from the street guts me emotionally by its
ESP of my conditions...I am so pleased that
I have been able to express such a purely
mental concept as thought-broadcasting by
the simple device of turning the brain into
a mouth.’
May 18: acutely disturbed. ‘My mind seems
to be thought-broadcasting very severely
and it is beyond my will to do anything
about it...I have summed this up by painting
my brain as an enormous mouth.’
April 29: Bryan has turmoil in his mind.
The features in his portrait have become
fragmented. He feels lonely and exposed,
as on a stage. ‘A strange spiritual force is
making me feel I should not smoke or I
will incur a disaster.’
June 27 (left): This is Bryan’s most complex
picture. He feels he is ‘closing in’ on the
essential image of schizophrenia. He feels
transparent. ‘I make crazy attempts at some sort
of control over what has become an impossible
situation (the man with the control stick). My
brain, my ego is transfixed by nails as the Christ
who could not move freely on the cross without
severe pain. So I find I cannot think without
feelings of pain.’ The red muzzled beast
symbolizes silent anger. ‘My senses are being
bent by fear into hallucinations.’

©2002 CRC Press LLC
REFERENCES
1.
Haslam J. Illustrations of Madness. London, 1810
2.
Kraepelin E. Psychiatrie: Ein Lehruch fur Studierende
und Arzte, 5th edn. Leipzig, Germany: JA Barth,
1896
3
Kraepelin E. Psychiatrie: Ein Lehruch fur Studierende
und Arzte, 6th edn. Leipzig, Germany: JA Barth,
1899
4.
Kraepelin E. Dementia Praecox and Paraphrenia
[1919]. Robertson GM, ed; Barclay RM, trans. New
York, NY: Robert E. Kreiger, 1971
5.
Bleuler E. Dementia Praecox or the Group of
Schizophrenias. Madison, CT: International Univer-
sities Press, 1950
6.
Schneider K. Clinical Psychopathology. Hamilton
MW, trans. London, UK: Grune and Stratton, 1959
7.
World Health Organization.
Report of the
International Pilot Study of Schizophrenia. Geneva:
WHO, 1979
8.
American Psychiatric Association. Diagnostic and
Statistical Manual, 4th Edition Revised (DSM–IV).
Washington, DC: APA, 1994
9.
World Health Organisation.
The International
Classification of Diseases, 10th Edition (ICD–10).
Geneva: WHO, 1992
10.
Jones P, Rodgers B, Murray R, et al. Child
development risk factors for adult schizophrenia in
the British 1946 birth cohort. Lancet 1994;344:
1398–1402
11.
Ciompi L. Catamnestic long-term study of the
course of life and aging in schizophrenia. Schizophr
Bull 1980;6:606–18
12.
Ciompi L. The natural history of schizophrenia in
the long term. Br J Psychiatry 1980;136:413–20
13.
Bleuler M. The long-term course of schizophrenic
psychoses. Psychol Med 1974;4:244–54
14.
Bland RC, Orn H. 14-year outcome in early
schizophrenia. Acta Psychiatr Scand 1978;58:327–38
15.
Salokangas RK. Prognostic implications of the sex of
schizophrenic patients. Br J Psychiatry 1983;142:
145–51
16.
Shepherd M, Watt D, Falloon I, et al. The natural
history of schizophrenia: a five-year follow-up study
of outcome prediction in a representative sample of
schizophrenics.
Psychol Med Monogr
1989;15
(Suppl.):1–46
17.
Frangou S, Murray RM. Schizophrenia. London:
Martin Dunitz, 1997
18.
Breier A, Schreiber JL, Dyer J, Pickar D. National
Institute of Mental Health longitudinal study of
chronic schizophrenia. Prognosis and predictors of
outcome. Arch Gen Psychiatry 1991;48:239–46
19.
Johnstone EC, Frith CD, Crow TJ, et al. The
Northwick Park ‘Functional’ psychoses study:
diagnosis and outcome. Psychol Med 1992;22:331–46
20.
Johnstone EC, Crow TJ, Frith CD, Owens DG. The
Northwick Park ‘Functional’ psychoses study:
diagnosis and treatment response. Lancet 1988;
2:119–25
21.
Loebel AD, Lieberman JA, Alvir JM, et al. Duration
of psychosis and outcome in first-episode schizo-
phrenia. Am J Psychiatry 1992;149:1183–8

©2002 CRC Press LLC
CHAPTER
2
Epidemiology and risk factors
The incidence of schizophrenia in industrialized
countries is in the region of 10–70 new cases per
100000 population per year
1
, and the lifetime risk
is 0.5–1%. The geographical distribution of
schizophrenia is not random: recent studies have
shown that there is an increased first-onset rate in
people born or brought up in inner cities (
Figure
2.1
)
2
. There is also a significant socioeconomic
gradient, with an increased prevalence in the
lower socioeconomic classes. ‘Social drift’, both in
social class, and into deprived areas of the inner
cities, may account for part of this, but specific
environmental risk factors (e.g. overcrowding,
drug abuse) may also be operating.
The onset of the disease is characteristically
between the ages of 20 and 39 years, but may
occur before puberty or be delayed until the
seventh or eighth decade. The peak age of onset is
20–28 years for men and 26–32 years for women
1
(
Figure 2.2
). The overall sex incidence is equal if
broad diagnostic criteria are used, but there is
some evidence for an excess in men if more
stringent diagnostic criteria, weighted towards the
more severe end of the diagnostic spectrum, are
Figure 2.1
Adjusted relative risk of schizo-
phrenia in Denmark according to place of
birth, with rural area used as the reference
category (*). Data from reference 2
0
Relative risk (95% Cl)
Capital
Suburb of capital
Provincial city
Provincial town
Rural area*
Greenland
Other countries
Unknown
1
2
3
4
5
6
7
RELATIVE RISK OF SCHIZOPHRENIA
ACCORDING TO PLACE OF BIRTH

©2002 CRC Press LLC
Figure 2.3
This graph is based on a
population cohort of 1.75 million
people from the civil registration
system in Denmark. The data
points and vertical bars show the
relative risks and 95% confidence
intervals, respectively, with the
month of birth analyzed as a
categorical variable. The curve
shows the relative risk as a fitted
sine function of the month of birth
(the reference category is
December). Figure reproduced
with permission from Mortensen
PB, Pedersen CB, Westergaard T,
et
al.
Effects of family history and
place and season of birth on the
risk of schizophrenia.
N Engl J Med
1.4
1.3
1.2
1.1
1.0
0.9
0.8
0.7
0.6
Relative risk
Month of birth
January
February
Ma
rch
April
May June
July
August
September
October
November
December
RELATIVE RISK OF SCHIZOPHRENIA
ACCORDING TO MONTH OF BIRTH
Figure 2.2
This graph shows the
incidence rate per 100 000 popu-
lation for broadly defined schizo-
phrenia in an inner city area of
London (Camberwell). Although
the overall rate is similar in males
and females, mean onset in women
is slightly later. Figure reproduced
with permission from Castle E,
Wessely S, Der G, Murray RM. The
incidence of operationally defined
schizophrenia in Camberwell
1965–84.
Br J Psychiatry
1991;159:790–4
60
50
40
30
20
76+
10
0
Rates per 100
000 population
Males
Females
Age at onset (years)
66–75
56–65
46–55
36–45
26–35
16–25
0–15
INCIDENCE OF SCHIZOPHRENIA BY GENDER

©2002 CRC Press LLC
applied. The prevalence of schizophrenia is consi-
derably higher in the unmarried of both sexes.
There is a small excess of patients born during the
late winter and early spring months in both north-
ern and southern hemispheres (and a less well-
known decrement in late summer (
Figure 2.3
)
2
.
People with schizophrenia have a twofold
increase in age-standardized mortality rates, and
are more likely to suffer from poor physical
health. Much of the increased mortality occurs in
the first few years after initial admission or diagn-
osis. Contributing factors early in the course
include suicide, with later factors, such as cardio-
vascular disorders, due in part to the poor lifestyle
of many patients, with heavy cigarette smoking
and obesity being common.
THE RISK FACTOR MODEL OF
SCHIZOPHRENIA
It is often said that schizophrenia is a disease of
unknown etiology. This is no longer true. Schizo-
phrenia is like other complex disorders such as
ischemic heart disease, which have no single cause
but are subject to a number of factors that
increase the risk of the disorder. Some of the risk
factors for schizophrenia are summarized in
Figure 2.4
. Schizophrenia, however, differs from
disorders such as ischemic heart disease in that we
do not understand the pathogenic mechanisms
linking the risk factors to the illness, i.e. we do not
understand how the causes ‘cause’ schizophrenia.
Figure 2.4
Causality over the life course. Risk factors for schizophrenia occur both early and late in
the life course, and interact with each other in a complex fashion
Psychosis
Childhood
vulnerability
Early causes
(genetic, obstetric
complications)
Late causes
(life events,
drug abuse)
Dysplastic
networks
Cognitive
impairment
Social difficulties
BIRTH ADOLESCENCE
THE DEVELOPMENTAL RISK FACTOR MODEL