ВУЗ: Не указан
Категория: Не указан
Дисциплина: Не указана
Добавлен: 02.10.2020
Просмотров: 2556
Скачиваний: 7
©2002 CRC Press LLC
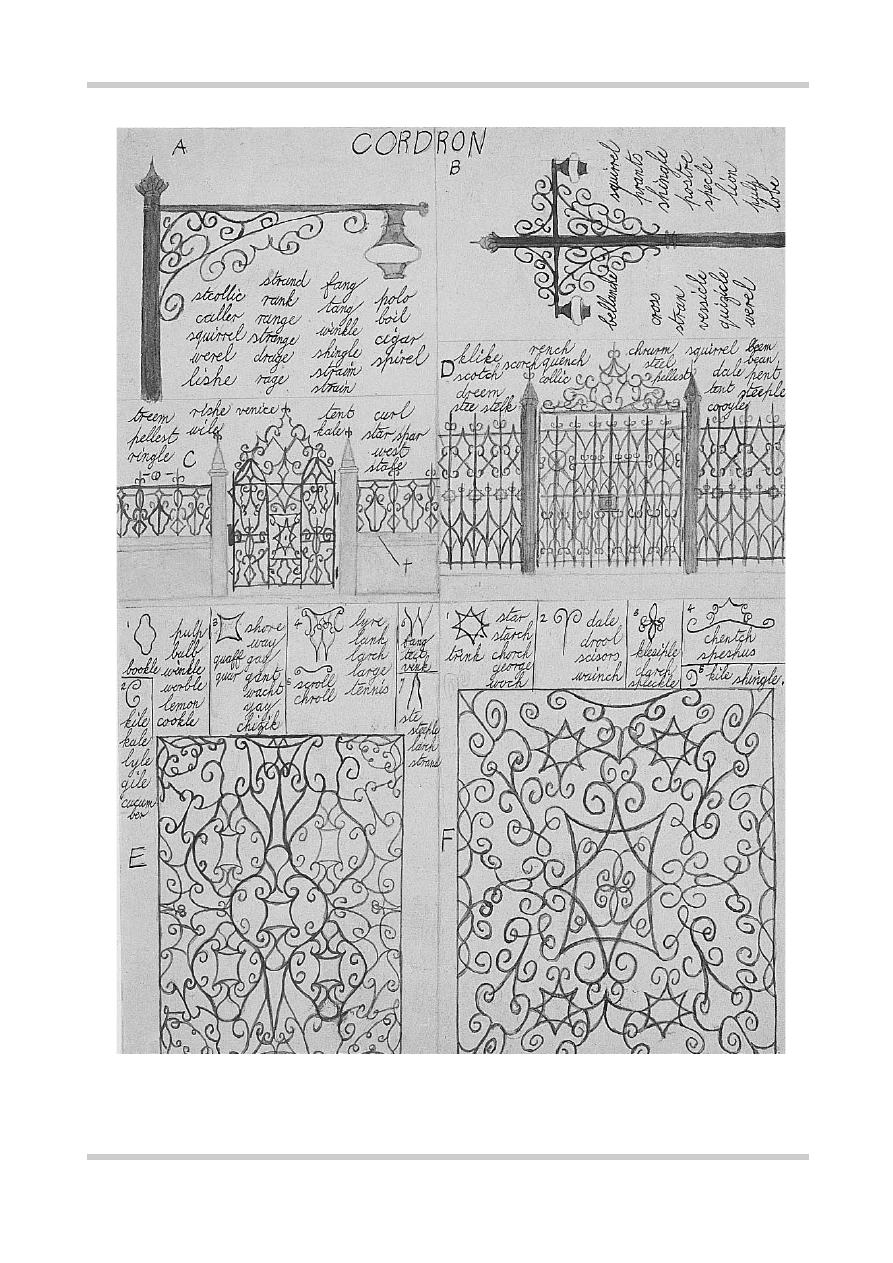
Figure 1.14
Cordron, by Gilbert Price. This patient was admitted at the age of 22 years. His extreme shyness and
eccentric behavior culminated in his arrest for ‘suspicious’ conduct. Neologisms, elaborated into complex
descriptive systems of pictures, chimneys and other objects, dominated his psychopathology. Reproduced with kind
permission of the Bethlem Royal Hospital Archives and Museum, Beckenham, Kent, UK
©2002 CRC Press LLC
Poverty of speech
Restriction in the amount
of spontaneous speech and in the information
contained in speech (alogia).
Flattening of affect
Restriction in the
experience and expression of emotion.
Anhedonia–asociality
Inability to experience
pleasure, few social contacts and social with-
drawal.
Avolition-apathy
Reduced drive, energy
and interest.
Attentional impairment
Inattentiveness at
work and interview.
NEGATIVE SYMPTOMS
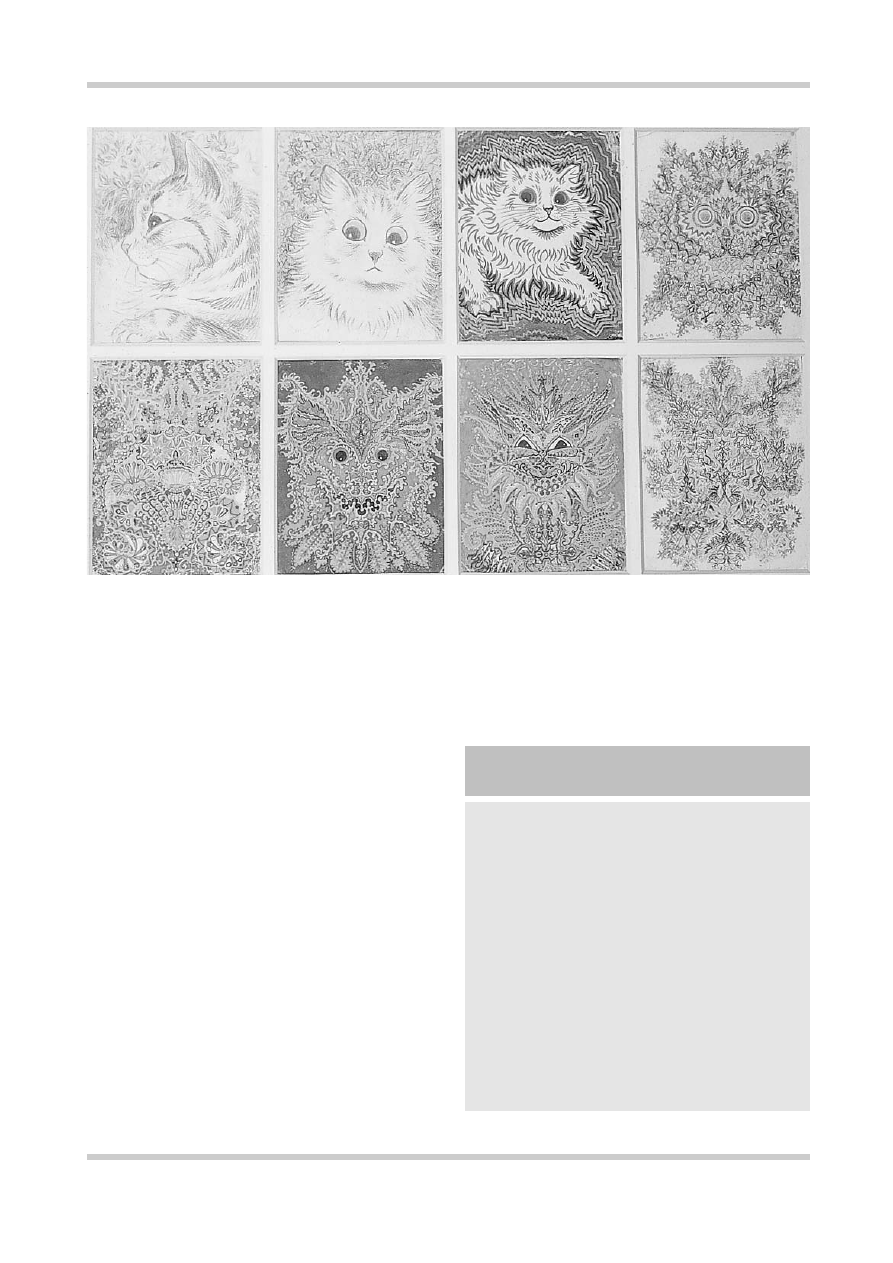
Figure 1.15
Cats, by Louis Wain (1860–1939). Wain was a British artist who became famous for his drawings of cats. He
was a patient at the Bethlem Hospital in the 1920s. Paintings such as these, which are suggestive of disorganization, visual
perceptual disturbances and abnormalities of affect, have been taken as illustrative of his psychological decline, although
more recent scholarship suggests that they were not out of keeping with contemporary design practice. Reproduced with kind
permission of the Bethlem Royal Hospital Archives and Museum, Beckenham, Kent, UK
THE CHRONIC ILLNESS
Eventually, even without treatment, the acute
symptoms of schizophrenia usually resolve.
Unfortunately this does not always mean that the
patient will fully recover. Over 50% of patients
diagnosed as suffering from schizophrenia will
show evidence of a significant degree of negative
symptomatology. Furthermore, in chronic schizo-
phrenia, positive symptoms also frequently
remain, although they tend not to predominate.
Negative symptoms may also be seen in the
acute episode, and their onset can often precede
(as one form of ‘schizophrenic prodrome’) the
development of typical positive symptoms.
Negative symptoms are multifactorial in origin.
Primary negative symptoms may be difficult to
distinguish from those secondary to florid positive

©2002 CRC Press LLC
and are the most important cause of long-term
disability.
COURSE AND OUTCOME OF
SCHIZOPHRENIA
The in-patient psychiatric population has fallen
dramatically since the 1950s in Western countries,
when effective antipsychotic drug treatments first
became available (
Figure 1.17
). However, the
outcome of schizophrenia, even with treatment,
remains variable (
Figure 1.18
and
Table 1.1
)
11–17
.
Longitudinally, the typical course of chronic
schizophrenia is described in
Figure 1.19
18
.
Schizophrenia also carries a high mortality. Rates
of suicide in follow-up studies vary from about 2%
psychotic symptomatology, while others may
represent side-effects of antipsychotic drugs. It is
often difficult to differentiate between the
negative symptoms of schizophrenia and the
symptoms of a depressive illness. Depression is
common in schizophrenia, and often becomes
evident as the acute episode resolves.
True primary negative symptoms are often
described as ‘deficit’ symptoms. Their frequency is
markedly increased in chronic schizophrenia and
is related to poor prognosis, poor response to
antipsychotic drugs, poor premorbid adjustment,
cognitive impairment and structural brain
abnormalities (sometimes called ‘type 2’ schizo-
phrenia). These symptoms are not easy to treat,
are often very distressing to families and carers,
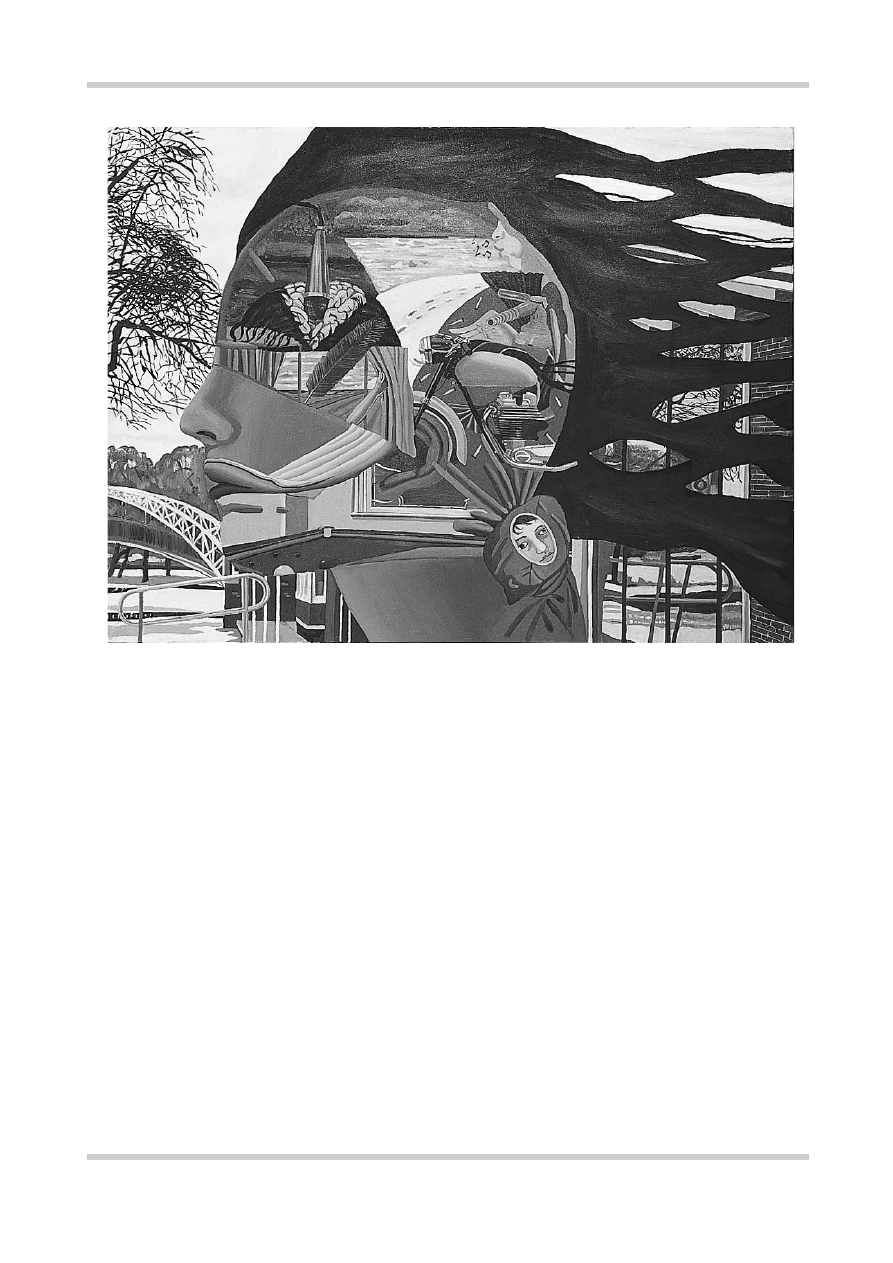
Figure 1.16
Broach shizophrene, by Bryan Charnley. Bryan Charnley illustrated the experience of psychosis in many
striking artworks, including a series of self-portraits painted as he came off medication (see
Figure 1.20
). Reproduced
with kind permission of the Bethlem Royal Hospital Archives and Museum, Beckenham, Kent, UK

©2002 CRC Press LLC
Figure 1.18
Course of schizo-
phrenia. Four typical patterns
in the course of schizophrenia
are described by Shepherd and
colleagues
16
who followed up
a cohort of patients with an
operational (CATEGO-defined)
diagnosis of schizophrenia who
were admitted to a UK hospital
over an 18-month period.
Figure reproduced with
permission from Shepherd M,
Watt D, Falloon I,
et al.
The
natural history of schizo-
phrenia: a five-year follow-up
study of outcome prediction in
a representative sample of
schizophrenics.
Psychol Med
Monogr
1989;15 (Suppl.):1–46
One episode
no impairment.
Several episodes with no
or minimal impairment.
Impairment after the first
episode with occasional
exacerbations of symptoms.
No return to normality.
Impairment increasing with
each exacerbation of
symptoms. No return
to normality.
13%
30%
10%
47%
1
2
3
4
FIVE-YEAR FOLLOW-UP OF 102 PATIENTS
WITH SCHIZOPHRENIA
160 000
140 000
120 000
100 000
80 000
60 000
40 000
20 000
0
1845
A
verage annual occupied
psychiatric hospital beds
185518651875188518951905191519251935194519551965197519851995
CHANGES IN THE IN-PATIENT PSYCHIATRIC
POPULATION OF ENGLAND & WALES
Figure 1.17
There was a steady
increase in the in-patient mental
hospital population in England and
Wales during the hundred years from
1860. This was due to a combination
of factors, including increased
urbanization and changes in mental
health legislation. The sharp decline
in this population coincided with the
introduction of effective antipsych-
otic medication, together with
changes in health policy and
legislation

©2002 CRC Press LLC
to 10% and the overall rate of suicide in schizo-
phrenia is estimated to be in the region of 10%
(
Figure 1.20
).
FACTORS AFFECTING PROGNOSIS
Certain clinical features are associated with a poor
prognosis: early or insidious onset, male sex,
negative symptoms
19,20
(
Figure 1.8
), lack of a
prominent affective component or clear precip-
itants, family history of schizophrenia, poor
premorbid personality, low IQ, low social class,
social isolation, and significant past psychiatric
history.
Several studies have demonstrated an
association between longer duration of untreated
illness and poorer outcome. For example, Loebel
and colleagues
21
found that a longer duration of
both psychotic and prodromal symptoms prior
to treatment was associated with a lesser likeli-
hood of remission. The longer the duration of
pretreatment psychotic symptoms, the longer
the time to remission. These data suggest that
early detection and intervention in schizo-
phrenia may be important in minimizing
subsequent disability.
Figure 1.19
Breier and colleagues
18
among others have
suggested that, despite the heterogeneity of schizophrenia,
a model of a common course of illness can be derived.
Based on evidence from their own studies and other long-
term follow-up studies they describe an earlier
deteriorating phase usually lasting some 5 years. During
this time there is a deterioration from premorbid levels of
functioning, often characterized by frank psychotic
relapses. After this phase much less fluctuation can be
expected and the illness enters a ‘stabilization’ or ‘plateau’
phase. This period may continue into the fifth decade,
when there is a third ‘improving’ phase for many patients.
Figure reproduced with permission from Breier A,
Schreiber JL, Dyer J, Pickar D. National Institute of Mental
Health longitudinal study of chronic schizophrenia.
Prognosis and predictors of outcome.
Arch Gen Psychiatry
1991;48:239–46
10
Years
Deteriorating
Course
20 30 40 50 60 70
Stable Improving
COURSE OF SCHIZOPHRENIA
(THEORETICAL MODEL)
Years of
follow-up
37
23
14
8
5
Number of
patients
289
208
90
161
49
Good clinical
outcome (%)
27
20
26
26
22
Poor clinical
outcome (%)
42
24
37
24
35
Social recovery
(%)
39
51
65
69
45
Study
Ciompi 1980
11,12
Bleuler 1978
13
Bland & Orne 1978
14
Salokangas 1983
15
Shepherd et al., 1989
16
Table 1.1 Summary of long-term clinical outcome studies in schizophrenia.
Table reproduced with permission from Frangou S, Murray RM.
Schizophrenia
. London: Martin Dunitz, 1997