ВУЗ: Не указан
Категория: Не указан
Дисциплина: Не указана
Добавлен: 02.10.2020
Просмотров: 2564
Скачиваний: 7

©2002 CRC Press LLC
patients as a group may be of lower birth weight
than the general population.
Neurodevelopmental abnormality
The morphological abnormalities that have been
reported in schizophrenia are consistent with a
neurodevelopmental event occurring in fetal or
early development. Some believe that the onset of
frank psychotic symptoms reflects the delayed
sequelae of an earlier developmental aberration,
which is then expressed as the brain continues to
develop in adolescence and adult life – sometimes
termed the ‘doomed from the womb’ view.
Delayed emergence of abnormal behavior
following lesions sustained during early develop-
ment is a well recognized phenomenon, and is
seen, for example, in animal models where ventral
hippocampal lesions, initially ‘silent’, are followed
by hyperactivity and increased responsiveness to
stressful stimuli and to dopamine blockade as the
animal matures. The inherited neurodevelop-
mental disease metachromatic leukodystrophy is
more likely to be associated with schizophreni-
form symptoms if the clinical onset is in
adolescence. In this case, as in schizophrenia, late
maturational events, such as myelination of
prefrontal nerve tracts and perforant pathway, or
abnormal synaptic plasticity, may reveal earlier
developmental abnormalities.
Later environmental factors
Substance misuse
The relationship between substance misuse and
schizophrenia is complex. Many drugs of abuse,
such as ketamine, amphetamine, cocaine, and
LSD, are psychotomimetic and can induce an
acute schizophrenia-like psychosis. Psychoactive
substance misuse both precedes and follows the
onset of psychotic symptoms. Some patients state
that they receive transient symptom relief and
are using the drugs as a form of ‘self-medication’.
However, it is also clear that abuse of certain
drugs can increase the risk of schizophrenia.
Evidence concerning cannabis comes from the
Swedish army study
19
in which army recruits
were interviewed about their drug consumption
and then followed-up for a decade and a half.
Those who admitted taking cannabis on more
than 50 occasions had a risk of later
schizophrenia some six times that of non-abusers
(
Figure 2.12
).
30
25
5
10
15
20
0
CANNABIS CONSUMPTION AT AGE 18
AND LATER RISK OF SCHIZOPHRENIA
Number of reported occasions
0
1
2–4 5–10 11–50 >50
Cases of schizoph
renia
(per 1000)
Figure 2.12
Substance
misuse can contribute to
later development of
schizophrenia. This study
following army recruits
found that those who
admitted taking cannabis on
more than 50 occasions had
a sixfold risk of schizo-
phrenia compared with
non-users. Figure reprod-
uced with permission from
Andreasson S, Allebeck P,
Engstrom A, Rydberg U.
Cannabis and
schizophrenia. A
longitudinal study of
Swedish conscripts.
Lancet
1987;2:1483–6

©2002 CRC Press LLC
It is estimated that 20–50% of the population
with schizophrenia in Western countries may
qualify as substance abusers or ‘dual-diagnosis’
patients. Such patients have a higher use of
services and worse outcome than patients who are
not abusers; they are more likely to be hospital-
ized and more likely to relapse. Patients with
schizophrenia seem to be more vulnerable to
significant harm at relatively lower levels of
substance use. As substance misuse is so prevalent
in the West, this is an area where secondary
prevention of relapse could be focused.
Social and psychological factors
Psychosocial factors appear to contribute to both
the onset and the relapse of schizophrenia. The
best documented are life events (
Figure 2.13
)
20
.
The effect size is smaller than in depression and
the time frame is somewhat shorter than in
depression (where adverse life events are well
recognized etiological factors), with the 3 weeks
prior to onset seeming to be the most important.
Unlike depression, all kinds of life events appear to
be important, not just those involving loss.
Many migrant groups show an increased first-
inception rate of schizophrenia compared both to
the population they have left and to that which
they have joined. The most striking example of
this is people of African-Caribbean origin living in
the UK (
Figure 2.14
)
1
. It seems unlikely that the
factors are biological. Odegaard
21
suggested in
1933 that social isolation and alienation are the
crucial factors, and most recent evidence points in
this direction.
CONCLUSION
There is no single cause for schizophrenia, rather a
number of risk factors (
Figure 2.15
) interact to
propel the individual over a threshold for
expression of the disease.
Figure 2.13
The rate of life
events is increased in schizo-
phrenia, although the effect is
not as great as in depression.
Figure reproduced with
permission from Bebbington
P, Wilkins S, Jones P,
et al.
Life events and psychosis.
Initial results from the
Camberwell Collaborative
Psychosis Study.
Br J
Psychiatry
1993;162:72–9
100
50
40
60
70
80
90
30
20
6
10
0
Life event rates per100 subjects
Months before onset/interview
5
4
3
2
1
Schizophrenia
Mania
Depressive psychosis
Controls
FREQUENCY OF LIFE EVENTS

©2002 CRC Press LLC
Figure 2.14
The differences in incidence in schizo-
phrenia in people of African-Caribbean origin
compared with those from other ethnic groups, in
one study from Camberwell, South London. Figure
reproduced with permission from Castle E, Wessely
S, Der G, Murray RM. The incidence of
operationally defined schizophrenia in Camberwell
1965–84.
Br J Psychiatry
1991;159:790–4
60
50
40
30
20
10
0
Rate per 10
0
000 population
All
African-
Caribbean
All other
ethnic
groups
ETHNICITY AND SCHIZOPHRENIA
Psychotic first-degree relative
Obstetric complications
Winter birth
City birth / upbringing
Cannabis use
Member of certain immigrant groups
Life events
RISK FACTORS AND EFFECT SIZES
(RR = 10)
Figure 2.15
There is no single
cause of schizophrenia. Instead,
like other complex disorders such
as coronary heart disease, a
number of genetic and
environmental factors interact to
cause the disease

©2002 CRC Press LLC
REFERENCES
1.
Castle E, Wessely S, Der G, Murray RM. The
incidence of operationally defined schizophrenia in
Camberwell 1965–84. Br J Psychiatry 1991;159:
790–4
2.
Mortensen PB, Pedersen CB, Westergaard T, et al.
Effects of family history and place and season of
birth on the risk of schizophrenia. N Engl J Med
1999;340:603–8
3.
Gottesman I, Irving I. Schizophrenia Genesis: The
Origin of Madness. New York, Oxford: WH Freeman,
1991:203
4.
Shields J, Gottesman II. Obstetric complications and
twin studies of schizophrenia: clarifications and
affirmations. Schizophr Bull 1977;3:351–4
5.
Kendell RE, Zealley AK. Companion to Psychiatric
Studies. Edinburgh: Churchill Livingstone, 1993
6.
Kringlen E. Twin studies in schizophrenia with
special emphasis on concordance figures. Am J Med
Genet 2000;97:4–11
7.
Fischer M. Genetic and environmental factors in
schizophrenia. A study of schizophrenic twins and
their families. Acta Psychiatr Scand 1973;238
(Suppl.):9–142
8.
Tienari P, Sorri A, Lahti I, et al. Genetic and
psychosocial factors in schizophrenia: the Finnish
Adoptive Family Study. Schizophr Bull 1987;13:
477–84
9.
Pollin W, Allen MG, Hoffer A, et al. Psychopathology
in 15,909 pairs of veteran twins: evidence for a
genetic factor in the pathogenesis of schizophrenia
and its relative absence in psychoneurosis. Am J
Psychiatry 1969;126:597–610
10.
Cardno AG, Marshall EJ, Coid B, et al. Heritability
estimates for psychotic disorders: the Maudsley twin
psychosis series. Arch Gen Psychiatry 1999;56:162–8
11.
Kety SS, Rosenthal D, Wender PH, Schulsinger F, et
al. Mental illness in the biological and adoptive
families of adopted schizophrenics. Am J Psychiatry
1971;128:302–6
12.
Rosenthal D, Wender PH, Kety SS, et al. The
adopted-away offspring of schizophrenics. Am J
Psychiatry 1971;128:307–11
13.
Pollack M, Woerner MG, Goodman W, Greenberg
IM. Childhood development patterns of hospitalized
adult schizophrenic and nonschizophrenic patients
and their siblings. Am J Orthopsychiatry 1966;36:
510–7
14.
Pearlson GD, Garbacz DJ, Moberg PJ, et al. Sympto-
matic, familial, perinatal, and social correlates of
computerized axial tomography (CAT) changes in
schizophrenics and bipolars. J Nerv Ment Dis 1985;
173:42–50
15.
Owen MJ, Lewis SW, Murray RM. Obstetric
complications and schizophrenia: a computed tomo-
graphic study. Psychol Med 1988;18:331–9
16.
O'Callaghan E, Gibson T, Colohan HA, et al. Risk of
schizophrenia in adults born after obstetric
complications and their association with early onset
of illness: a controlled study. Br Med J 1992;305:
1256–9
17.
O'Callaghan E, Larkin C, Kinsella A, Waddington JL.
Obstetric complications, the putative familial-
sporadic distinction, and tardive dyskinesia in schizo-
phrenia. Br J Psychiatry 1990;157:578–84
18.
Susser E, Neugebauer R, Hoek HW, et al.
Schizophrenia after prenatal famine:
further
evidence. Arch Gen Psychiatry 1996;53:25–31
19.
Andreasson S, Allebeck P, Engstrom A, Rydberg U.
Cannabis and schizophrenia. A longitudinal study of
Swedish conscripts. Lancet 1987;2:1483–6
20.
Bebbington P, Wilkins S, Jones P, et al. Life events
and psychosis. Initial results from the Camberwell
Collaborative Psychosis Study. Br J Psychiatry 1993;
162:72–9
21.
Odegaard S. Emigration and insanity. Acta Psychiatr
Scand 1932;Suppl. 4
©2002 CRC Press LLC
CHAPTER
3
Pathogenesis
Pathogenetic theories need to encompass all levels
of brain structure and function, from the basic
neuroanatomical level, through neurochemical,
neurophysiological and neuropsychological find-
ings, and thence through to symptoms. As yet, we
have only a very partial understanding of these
mechanisms.
STRUCTURAL IMAGING AND ANATOMICAL
STUDIES
The core brain structural finding in schizophrenia,
of lateral ventricular enlargement (
Figure 3.1
) is
now well established, but the degree of enlarge-
ment is relatively small (
Figure 3.2
); about 25% on
average
1
. Monozygotic twins discordant for
schizophrenia can be distinguished from their co-
twins on the basis of ventriculomegaly and
decreased temporal cortical volume (
Figure 3.3
)
2
.
Numerous other morphological abnormalities
have been reported (
Figures 3.4
3
and
3.5
). People
with schizophrenia appear to have very slightly
smaller brains with sulcal widening and reduced
cortical volume, particularly in the temporal lobes.
A number of other findings have been
reported. Most of these are non-specific and tell us
little about pathogenesis, but there are some clues
to the processes that might be involved. Normally
rare developmental abnormalities, such as agenesis
of the corpus callosum (
Figure 3.6
), aqueduct
stenosis, cavum septum pellucidum, cerebral
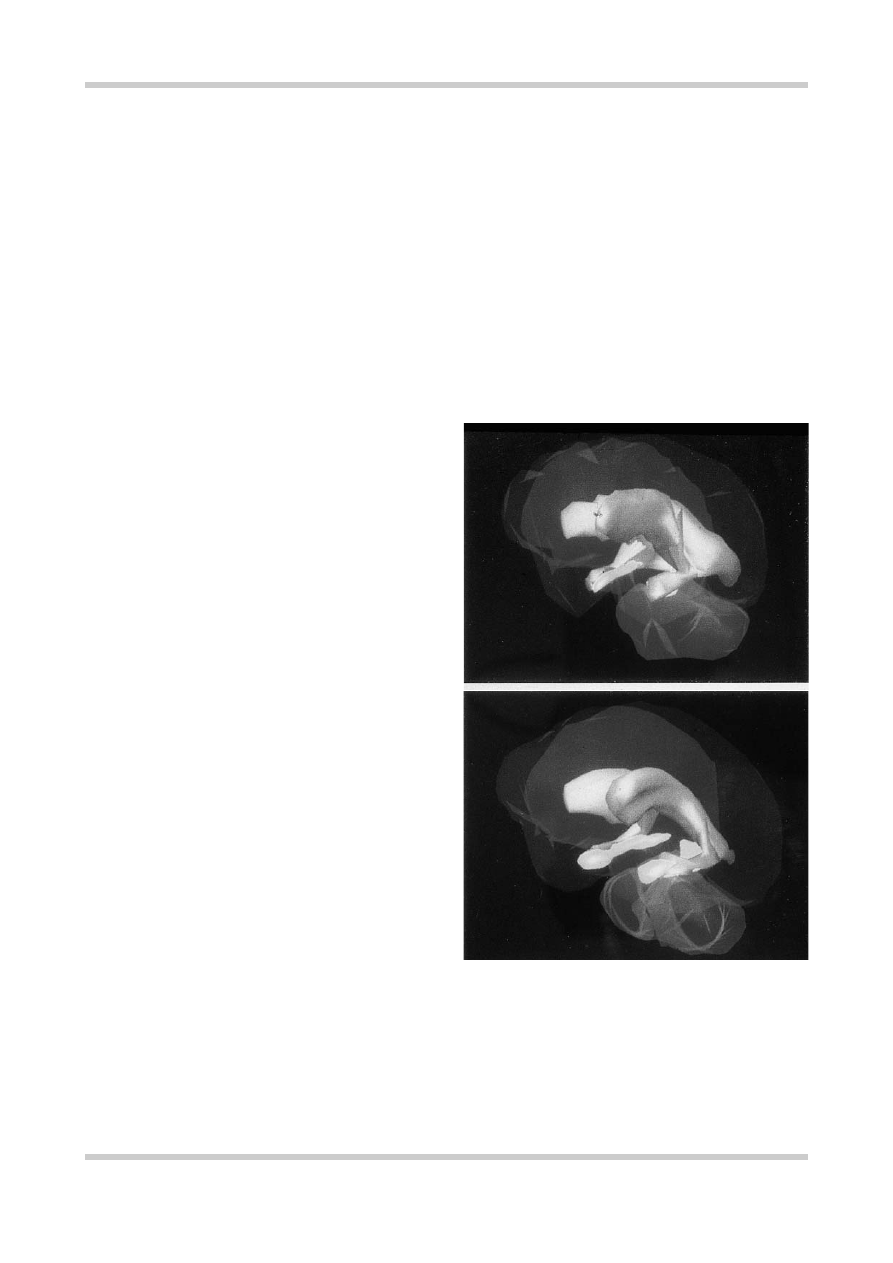
Figure 3.1
Three-dimensional reconstruction of the
ventricular system in schizophrenia. Structural changes
appear in the shrunken hippocampus (yellow) and enlarged
fluid-filled ventricles (gray) of the brain of a patient with
schizophrenia (a) compared with that of a healthy volunteer
(b). Figure reproduced with kind permission of Professor
Nancy C. Andreasen, University of Iowa, USA
b
a